The Quick & Dirty Guide to Poisonings

A "poison" is defined as a substance that can produce harmful physiological or psychological effects when ingested, inhaled, injected or absorbed through the skin. Poisoning emergencies are a major cause of morbidity and mortality in the US; responsible for 10% of all EMS calls annually, according to the National Safety Council (NSC). To assist with the serious problem of poisonings, there are 60 poison control centers around the country, answering the call for assistance, 24 hours a day, 7 days a week. The centers report a staggering 4.7 million calls a year within the continental United States. Regional poison control centers are a ready source of information for any toxicological emergency. Depending on your local protocols, poison control centers may be contacted directly by EMS personnel, or through the regional medical command center. Either way, they are always there to assist. The immediate determination of potential toxicity is based on:
- The specific agent involved
- The amount of the substance ingested
- The route of exposure
- The time it was ingested
- The presence of signs/symptoms of toxicity
- The patient's overall condition
- The initial EMS findings/treatment
Poisoning by Ingestion

More than 80% of all accidental poisonings occur from ingestions that occur in children 1 -3-year-olds. Children at this age, learn and explore new things by putting them in their mouths thereby, accidentally swallowing the potential poison. The most common exposures in this group are from household products. Adult poisonings, on the other hand, are usually intentional, although a small percentage do occur accidentally by chemical exposures while at work. Deliberate poisonings are often an act of a desperate patient attempting suicide, more often than homicide attempts by 10 to 1.
Either way, intentional poisonings must be reported to the proper authority, by EMS personnel in all jurisdictions within the US. The toxic effects of an ingested poison may be immediate or delayed, depending on the poison, and the amount.
Patient findings that may point to a potential poisoning include:
- Decreased level of consciousness
- Airway compromise/injury from chemical burns/edema, a mouthful of pills, etc.
- Abnormal respiratory patterns/potential for agonal respirations
- Dysrhythmias that usually affect the rate (tachycardia, bradycardia)
- Combative/intoxication/delirium
The EMT must consider possible poisoning, anytime a patient's condition can't be attributed to other explainable causes (i.e., hypoglycemia, hyperglycemia, and cardiac dysfunction)
Respiratory Complications
The first priority (of course, after scene safety is established) in managing a poisoned patient is to provide adequate ventilatory support, as it is needed (PRN). Spontaneously breathing patients with a sufficient tidal volume should receive high concentration O2 therapy; while some patients may not be able to protect their airway, requiring an advanced airway adjunct and ventilatory support with a BVM and 100% O2, to prevent hypoxemia and aspiration. Other respiratory conditions that may be associated with a poisoning patient include, the early development of non-cardiogenic pulmonary edema or the later development of adult respiratory distress syndrome (ARDS). Bronchospasm is common with a poisoning patient and may be caused by direct or indirect effects of the toxin.
Cardiovascular Complications
Common cardiovascular complications seen in ingested poison patients are cardiac dysrhythmias. It is essential to assess the patient's circulatory status and continually monitor the patient for dysrhythmias on the monitor. The presence of tachydysrhythmias/bradydysrhythmias, may indicate the presence of severe disorders caused by the toxin, such as acidosis and hypoxia/hypoxemia. It is essential for the EMT to closely monitor the patients BP; it is common for toxins to cause hypotension, by decreasing vascular tone. Rarely, hypertension may develop after a toxic ingestion, leading to a cerebrovascular hemorrhage.
Neurological Complications
The EMT should perform and record a baseline neurological exam. Deviations from a normal sensorium can range from mild drowsiness to agitation, hallucinations, seizures, coma, and death. Neurological complications may arise from the toxin itself, as seen with children that ingest paint chips and develop lead poisoning. Complications may also arise as a metabolic or perfusion disorder.
History
The EMT must obtain a pertinent history of the exposure and any relevant past medical history, when at all possible from the family or patient. Expect the information to be unreliable though, especially in cases involving children, drug use, or suicide attempts but, regardless the EMT should determine the following information, if possible:
- What substance was ingested? (Obtain the container or remaining poison if safe to do so)
- When was the substance ingested? (This answer may affect the determination to use activated charcoal, gastric lavage, or to administer an antidote)
- How much of the substance ingested?
- Was there an attempt to vomit or did the patient vomit prior to EMS arrival?
- Has an antidote or activated charcoal or Ipecac administered prior to EMS arrival?
- Does the patient have a psychiatric history pertinent to suicide attempts or any recent depression?
Gastrointestinal Decontamination
One important goal of managing serious poisonings is to prevent the specific toxin from reaching the small intestines and to limit its absorption. This may be attempted by gastric decontamination, through the use of antidotes, and sometimes gastric lavage depending on local protocol. Before attempting to remove a poison from the gastrointestinal tract, consult medical command or poison control for direction.
Note: Activated charcoal use alone for neutralizing/removing poisons from the gastrointestinal tract is considered equivalent or superior to other means and has fewer complications.
Activated Charcoal
Activated charcoal is an inert, nontoxic product of wood material that has been heated to high temperatures. It is able to adsorb (collect in a condensed form) molecules of any chemical toxins while in the intestinal tract. The charcoal reduces the absorption of the poison by as much as 50% and prevents its absorption into body systems. It is a safe and effective treatment for most toxic ingestion's as listed below:
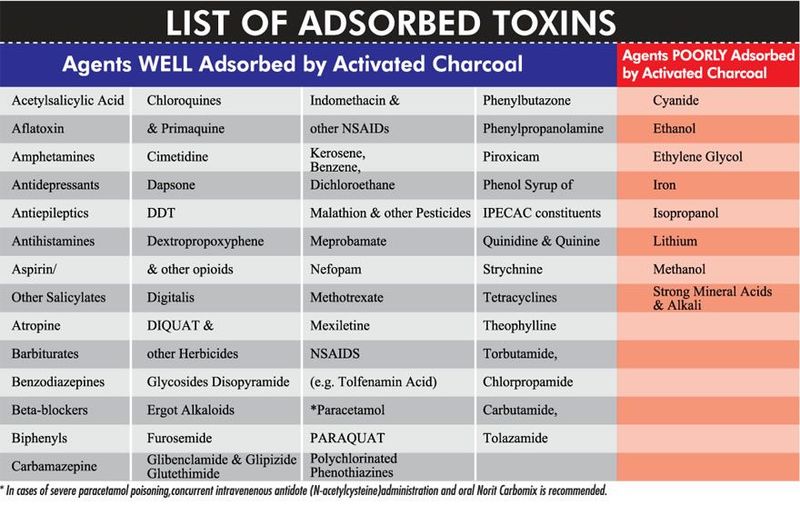
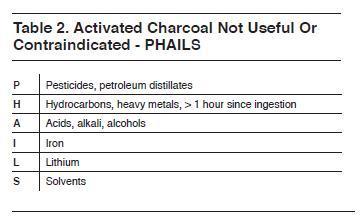
If any of these substances have been ingested, it is advisable for the paramedic to withhold activated charcoal and contact medical command/poison control. Activated charcoal should also be withheld when the ingested agent has a specific antidote available (i.e., N-acetylcysteine for acetaminophen overdose; Naloxone for narcotic overdose). Activated charcoal is most effective when administered within the first hour after ingestion of the toxin. After 1 hour, the toxin has more than likely entered the small intestine; where activated charcoal does not reach!
Note: Activated charcoal should be withheld when the toxic ingestion occurred longer than 1 hour before EMS arrival!

Activated charcoal comes in an aqueous solution with or with or without a cathartic. A cathartic is an agent that is added to cause quicker bowel evacuation for the charcoal and its binding. Activated Charcoal complications include the unwillingness of patients to consume the activated charcoal, especially children. Some manufacturers are now adding flavors to try to make them more appealing to the patient. Another possible complication is that it may induce vomiting, causing charcoal to be expelled on the patient, your unit, and you so be prepared for a possible mess whenever charcoal is involved.
Syrup of Ipecac
(NO LONGER ACCEPTABLE TO ADMINISTER BY EMS)
Note: Syrup of Ipecac is no longer used in the pre-hospital/hospital setting, it is only discussed here because it may still be used prior to EMS arrival, so a general knowledge is needed.
Syrup of Ipecac was once widely used by EMS to prevent the absorption of poison, but recent studies show that ipecac only reduces absorption by 30%, at best; it may also interfere with the effectiveness of other means of decontamination such as activated charcoal. It may also cause the patient to have a higher incidence of aspiration than seen with other treatments. The possible complications are severe and include:
- Mallory-Weiss esophageal tears of the esophagus
- Pneumo-mediastinum (air or gas within the mediastinum)
- Fatal diaphragmatic/gastric rupture
- Aspiration pneumonitis
Syrup of Ipecac is no longer acceptable to be used in the pre-hospital environment; Protocols now replace Ipecac with the words
"Do Not Induce Vomiting"
Gastric Lavage

Gastric lavage is an approved method of gastrointestinal decontamination and offers the ability to rapidly remove most of the gastric contents. Especially, if the lavage is performed with charcoal and within the first hour of the toxic ingestion (while the potential toxin remains in the stomach). Gastric lavage is also an excellent route for the administration of activated charcoal without causing the patient to gag on the grittiness of the charcoal. Gastric lavage is usually performed with a large-bore orogastric 36 to 40 French for adults and 24 to 28 for children rather than using a smaller nasogastric tube. The smaller lumen may not allow for the evacuation of larger stomach particles (i.e., half dissolved pills/large particle toxin).
Note: Never try to use an orogastric tube in the nasal cavity, it will probably cause epistaxis and mucosa damage to the patient.
The proper procedure for gastric lavage:
- If the patient is conscious; place them in the left lateral Trendelenburg position, some may call it the "swimmer's position". This position can aid in the prevention of aspiration if vomiting occurs, and it may believe it!
Note: Endotracheal intubation should precede gastric lavage in patients that are unconscious, that have an altered level of consciousness, or patients without an intact gag reflex. - Gently, insert the orogastric tube through the mouth and into the patient's esophagus, continue to advance the tube until it reaches the stomach.
Note: If the EMT meets resistance while advancing the tube into the stomach, the procedure should be aborted and contact medical command. - Check for proper tube placement before lavage begins, by injecting air into the orogastric tube with a 60 cc syringe while auscultating over the epigastric region for a gurgling/bubbling sound as air enters the stomach.
- To reaffirm placement, aspirate some of the gastric contents with the attached 60 cc syringe.
- Infuse normal saline (tap water can be used, but it is best to use saline when possible) in amounts not to exceed 150 mL to 200 mL in adults and 50 to 100 mL. in children under 5 years old.
Note: To prevent water absorption and resultant fluid-electrolyte imbalances in pediatric/geriatric patients; only normal saline should be used for gastric lavage. - Continue gastric lavage until the return of fluid is clear.
Note: The total fluid return should be close to the same amount that was infused
Gastric lavage is contraindicated in patients:
- That can not protect their own airway
- Have an altered level of consciousness without intubation
- Have ingested low viscosity hydrocarbons:
- Gasoline
- Kerosene
- Furniture polish
- Mineral spirits - Have ingested a possible caustic agent
Patients with an altered level of consciousness can receive gastric lavage, as long as the patient has been successfully intubated prior to the evacuation procedure. Patients that have suffered a toxic ingestion, should be intubated using rapid sequence intubation procedures when local protocol and the EMT's level of training allows it.
Possible complications of an orogastric tube insertion although rare do exist; they include:
- Accidental tracheal insertion of the orogastric tube
- Esophageal perforation
- Aspiration
- Pneumonitis
- Fluid/electrolyte imbalances
Managing Specific Toxic Agents
EMS treatment is centered on managing the specific signs and symptoms and stopping or slowing the absorption of the toxin.
There are few antidotes that are effective for ingested poisons, they include:
Antidotes for Common Toxins |
|
TOXIN |
ANTIDOTE |
Acetaminophen |
N-acetylcysteine |
Anticholinergic agent |
Physostigmine |
Benzodiazepine |
Flumazenil |
Beta-Blocker |
Glucagon |
Calcium Channel Blocker |
Calcium |
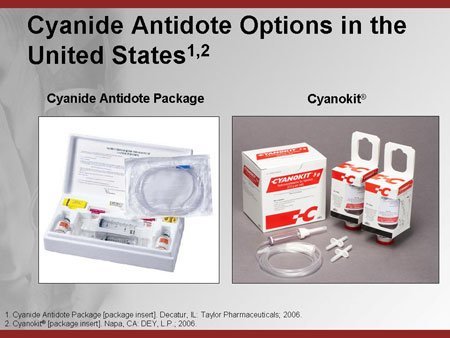
Cyanide |
Hydroxocobalamin (Cyanokit), Sodium Thiosulfate |
Cyclic Antidepressant |
Bicarbonate |
Digoxin |
Digoxin immune Fab |
Iron |
Deferoxamine |
Methanol |
Ethanol |
Opiate |
Naloxone |
Organophosphate |
Atropine, Pralidoxime |
Strong Acids and Alkalis
Strong acids and alkalis can cause severe burns to the mouth, pharynx, esophagus and sometimes the upper airway and gastrointestinal tracts on contact. Perforation of the esophagus or stomach may result in vascular collapse, mediastinitis (inflammation of the mediastinum), and Pneumo-peritoneum (air or gas in the peritoneal cavity of the abdomen). The frequency of caustic ingestion is higher in small children and is usually caused by lye; accounting for a large percentage of all toxic ingestions annually. Acids commonly complete their damage on tissue, within 1 or 2 minutes of contact. However, alkalis (especially solid alkalis) may continue to cause liquefaction of tissues for minutes to hours, causing extreme damage.
Therefore, EMS treatment of these patients is mainly supportive, IV administration of fluids and rapid, safe transport to the nearest appropriate facility for definitive treatment. In an adult patient, with the medical command/MCP direction, it is appropriate to give 200 to 300 cc of an approved fluid (WATER & MILK ONLY!), while in children, the recommendation is up to 15 mL/kg (that would be the maximum).
Note: Efforts to neutralize the ingested toxin with anything other than water or milk is contraindicated, Some common juices and vinegar can cause exothermic reactions, causing burns.
Common Acid and Alkali Substances
|
|
ACID |
ALKALI |
Acetic acid |
Ammonia |
Battery acid |
Bleach |
Disinfectants with bleach |
Disk batteries |
Hydrochloric acid |
Toilet bowl cleaner |
Metal Cleaners |
Hair dyes/tint |
Phenol |
Jewelry cleaner |
Sulfuric acid |
Metal cleaner/polish |
Swimming pool cleaners |
Paint remover |
Toilet bowl cleaners |
Sodium or potassium hydroxide (lye) |
|
|
Washing powder (clothing) |
Hydrocarbons
Hydrocarbons are a group of saturated and unsaturated compounds that are mainly derived from crude oil, coal, or plant sources. Mixtures of these agents vary in viscosity and volatility, which is their resistance to flow and ability to vaporize. These two attributes, along with other factors, determine the toxic effect of the individual agent. Other factors include surface tension, the presence of other chemicals within the toxic product, total amount and route of the exposure. Hydrocarbons are found in household cleaners therefore, toxic ingestion by children is common.
The most important physical characteristic in the potential toxicity of ingestion is its viscosity; the lower the viscosity, the thinner the liquid. The thinner the liquid the more potential for aspiration and deep gastrointestinal burns. The more volatile compounds become gases when they come in contact with wet mucosa membranes. The clinical features of hydrocarbon ingestion vary widely depending on the type of agent involved.
If the patient is not displaying symptoms, then it is a safe bet, that the chances of a serious complication from hydrocarbon exposure is very low. However, any patient that is coughing, choking, or has spontaneous emesis when trying to swallow should be treated as if a hydrocarbon aspiration has occurred until proven otherwise. Hydrocarbon ingestion may involve the patients' respiratory, gastrointestinal, and neurological systems.
Managing Hydrocarbon Poisoning:
- Ensure an adequate airway while providing ventilatory and circulatory support, as needed.
- Identify the substance involved if at all possible. Contact medical command/poison control.
- Gastrointestinal decon of the stomach is normally contraindicated in these patients to prevent pneumonitis. Medical command/MCP may recommend gastric emptying if a petroleum product is involved. In this case, the risk of systemic toxicity is greater than the risk of aspiration. Activated charcoal and other diluents have not been shown to be effective with hydrocarbon ingestion.
- Initiate IV therapy with normal saline and bolus or run IV, per MCP recommendations.
- Monitor cardiac rhythm for the development of dysrhythmias.
- Rapid, safe transport in the left lateral recumbent position with the head elevated, if possible, to prevent emesis.
Methanol
Methanol, aka wood alcohol, is a common industrial solvent that is obtained from the distillation of wood. Methanol is actually a poisonous alcohol found in a variety of products that are found around the house. The main difference with other toxins is the ability of hydrocarbons to be ingested orally, absorbed or inhaled. Methanol itself is no more toxic than ethanol, however, its metabolites are extremely toxic. As it is absorbed, it is converted in the liver to form formaldehyde, and within minutes, it forms formic acid, which causes, you got it, massive metabolic acidosis. As the toxins accumulate in the blood, it causes a group of symptoms related to CNS depression.
The symptoms correlate with the degree of acidosis and may include the following:
- CNS Depression
- Lethargy
- Confusion
- Coma
- Seizures - Gastrointestinal Tract
- Nausea & Vomiting
- Abdominal Pain - Visual Complaints
- Photophobia
- Blurred vision
- Dilated/Sluggish Pupils
- Seeing Spots
- Blindness ( can occur with as little as 4 oz. ingestion) - Metabolic Acidosis
Shortness of Breath
- Tachypnea
- Shock
- Multi-system failure/shut down
- Death
Managing Methanol Poisoning
- ALS Supportive Care: Ensure an adequate airway while providing ventilatory and circulatory support, as needed. (Adequate oxygenation is needed to help correct acidosis and maximize respiratory excretion). Establish IV access with normal saline (per medical command/protocol).
- Gastrointestinal Decontamination: If it has been within the "golden" hour of ingestion; gastric lavage may be indicated. The use of activated charcoal is controversial, so contact medical command for proper protocol.
- Correction of Metabolic Acidosis: MCP/Medical control may recommend trying sodium bicarbonate to correct the acidosis, depending on local protocols. Large and/or repeated doses may be indicated to neutralize methanol and serum formic acid. Hemodialysis will probably be performed, once the patient arrives at the hospital.
- Preventing methanol from converting to formic acid: This may be accomplished by administering ethanol, that's right, booze! It has a 9 times greater affinity for the enzyme that creates formic acid. If the patient is conscious, administer 30 to 60 cc of 80 proof ethanol by mouth or gastric lavage tubing. Unconscious patients can receive the same treatment except they must be intubated and the ethanol must be administered by orogastric tube.
- Rapid, Safe Transport: Provide a rapid, safe transport to the nearest appropriate medical facility with the capabilities to deliver definitive care.
Ethylene Glycol
Ethylene glycol is a colorless, odorless, water-soluble liquid that is commonly used automotive products. The accidental ingestion in children is common because of its appealing colors and warm, sweet flavor. The products are commonly misused by alcoholics in the substitution of ethanol. As little as 60 cc can be lethal in adults and much less for children. Early signs and symptoms of CNS depression are caused by the ethanol like effects of the ethylene glycol. However, toxicity from ethylene glycol and methanol is caused by the build-up of glycolic and oxalic acids in the liver and kidneys, after metabolism. The acids may affect the CNS, cardiopulmonary, and renal systems and can cause the development of hypocalcemia.
The main signs and symptoms of ethylene glycol poisoning generally occur in 3 stages. Although EMS will only be concerned with stage I, it is important to see the progression in cases of delayed EMS treatment.:
Stage I: CNS effects occurring within the first 12 hours after ingestion:
- Slurred speech
- Ataxia
- Somnolence
- Nausea and vomiting
- Focal/general convulsions
- Hallucinations
- Stupor
- Coma
Stage II: Cardiopulmonary system effects occurring 12 to 36 hours after ingestion:
- Rapidly progressing tachypnea
- Cyanosis
- Pulmonary edema
- Heart Failure
Stage III: Renal system effects occurring 24 to 72 hours after ingestion:
- Flank pain
- Oliguria
- Hematuria
- Uremia
Managing Ethylene Glycol Poisoning:
The emergency care for ethylene glycol poisoning is similar to methanol treatment, which includes the following:
- ALS Supportive Care: Ensure an adequate airway while providing ventilatory and circulatory support, as needed. (Adequate oxygenation is needed to help correct acidosis and maximize respiratory excretion). Establish IV access with normal saline (per medical command/protocol).
- Gastrointestinal Decontamination: If it has been within the "golden" hour of ingestion; gastric lavage with activated charcoal may be indicated (contact MCP/medical command). Charcoal may decrease ethylene glycol absorption by 50%.
- Ensure Renal Function: Initiate IV therapy with a volume expanding fluid to maintain adequate urine output.
- Administer Sodium Bicarbonate IV (check local protocol).
- Prevent ethylene glycol from converting to a toxic acid: This may be accomplished by administering ethanol (30-60 cc) by mouth or preferably via the orogastric tube. This will block the conversion of ethylene into a toxic acid by metabolism. Unmetabolized ethylene glycol is excreted by the lungs and kidneys.
- Rapid, Safe Transport: Provide a rapid, safe transport to the nearest appropriate medical facility with the capabilities to deliver definitive care.
Special Note: EMS should expect to be ordered by medical command physician or poison control to administer the following medications in some instances:
- Thiamine to degrade glycolic acid to a nontoxic metabolite
- Calcium Gluconate or Calcium Chloride to manage possible hypocalcemia
- Diazepam or Lorazepam to control active seizure
Isopropanol
Isopropanol (isopropyl alcohol) is a colorless volatile, flammable liquid that has a bittersweet taste. It is common ingredient in rubbing alcohol and other household agents. The common routes of toxic exposure include intentional consumption, accidental ingestion and inhalation of large amounts of the vapor. Isopropanol is more toxic than ethanol and less toxic than methanol or ethylene glycol. A potential fatal dose in an adult patient would be in the 150 to 240 cc range depending on the person. In children, any amount of isopropanol is considered potentially toxic.
After ingestion, 80% of the isopropanol is converted to acetone and the rest is excreted unchanged by the kidneys. The remaining acetone is then excreted by the kidneys and to a lesser, slower extent the lungs. Isopropanol poisoning affects several body systems including the CNS, gastrointestinal, and renal systems. Isopropanol is 2 to 3 times more potent of a CNS and respiratory depressant than ethanol.
The signs and symptoms often occur within 30 minutes after ingestion and include the following:
- Respiratory depression
- CNS depression
- Abdominal pain
- Gastritis
- Hematemesis
- Hypovolemia
Managing Isopropanol Poisoning
- ALS Supportive Care: Ensure an adequate airway while providing ventilatory and circulatory support, as needed. (Adequate ventilation is needed to help maximize respiratory excretion to eliminate acetone). Establish IV access with normal saline (per medical command/protocol) and provide fluid resuscitation as needed.
- Gastrointestinal Decontamination: If it has been within the "golden" hour of ingestion; gastric lavage may be helpful although isopropanol is also secreted in salivary glands and stomach.
- Rapid, Safe Transport: Provide a rapid, safe transport to the nearest appropriate medical facility with the capabilities to deliver definitive care.
Note: In this case, the administration of ethanol will not prevent the toxic build-up of acids from metabolism to the same effective degree as in the methanol and ethylene glycol treatment modality.
Metals
Infants and young children are at high risk for unintentional iron, lead, and mercury poisonings. Their immature immune system and increased absorption as a normal function of their age contribute greatly to the risk of exposure. Unintentional/intentional ingestion of iron can be fatal; causing gastrointestinal hemorrhage and bloody vomitus, painless bloody diarrhea. The more severe exposures occur when ingestion amounts exceed 20 mg/kg. In such cases, death can occur within 12 to 48 hours after ingestion, although most people survive ingestion of iron.
Managing Metal Poisoning
- ALS Supportive Care: Ensure an adequate airway while providing ventilatory and circulatory support, as needed. Establish IV access with normal saline (per medical command/protocol) and provide fluid resuscitation as needed.
- Gastrointestinal Decontamination: Is normally withheld until physician evaluation in the ER, but is usually conducted in order to prevent further absorption.
- Rapid, Safe Transport: Provide rapid, safe transport to the nearest appropriate medical facility with the capabilities to deliver definitive care.
Cyanide
Cyanide refers to any of a number of highly toxic substances that contain the cyanogen chemical group. Because of its toxicity, cyanide is less used in products than it used to be. The agent is still sometimes seen in ore extraction, electroplating, and as a fertilizer. Cyanide is a product of combustion from burning many products, including nylon. Therefore cyanide poisoning is possible in and around house fires. Cyanide may be inhaled or ingested in the form of cyanide salts, nitrites, or cyanogenic glycosides. It combines and reacts with ions to inhibit cellular oxygenation. The hypoxic state progresses quickly from dyspnea to paralysis, unconsciousness, and death. Large doses are normally fatal rapidly from respiratory arrest.
Managing Cyanide Poisoning
- Don the proper BSI as needed, to prevent possible rescuer contamination.
- Remove the patient from the hazard, if it is still present. Decontamination and clothing removal is key to stopping the potential spread of cyanide poisoning.
- Ensure a patent airway and provide ventilatory support as needed. Anticipate the need for an advanced airway if thermal injury is evident to the airway.
- Administer high-flow O2 and monitor closely for worsening signs of hypoxia.
- If using a Cyanokit (Hydroxocobalamin), contact medical command/poison control and follow instructions provided with the kit (if local protocol/medical command will allow). These are now carried on many ground EMS and air medical units.
- Initiate IV therapy with a volume-expanding fluid. Be careful not to overload the patient with fluids, especially if this is an ingestion/inhalation patient and not a burn patient.
- Monitor cardiac rhythm, observing for the presence of ectopy or dysrhythmia to develop.
- Provide safe, rapid transport to an appropriate medical facility for definitive treatment.
Poisonings and Toxic Ingestions
Now that you've pounded the poison guide, it's time to challenge yourself: