Test Complete
- Questions
- Score
- Minutes
| Overall Results | |
|---|---|
| Total Questions |
| Category Results | |
|---|---|
Secondary Assessment
Category: Medical
Topic: Basic Medical Assessment
Level: EMT
Next Unit: Family History Risk Factors
11 minute read
Complete secondary assessments may or may not be appropriate to perform on all medical patients and are designed to identify any signs or symptoms of illness that may not have been revealed during the initial assessment. Emergent situations may be time-sensitive and focused only on the highest quality pre-hospital care, which at times may prevent the luxury of a complete secondary assessment.
However, when time and situation allow, and when appropriate, the secondary assessment includes:
SKIN: Observe for rashes or blisters and whether they follow a dermatome. Petechiae and ecchymoses should be identified.
HEAD: The head and scalp should be assessed for pain and symmetry. The face should be assessed for pain and symmetry of facial muscles.
In cases of suspected stroke, symmetry also includes evaluating the tongue to see if it deviates when asking the patient to stick it out.
A pulmonary complaint in the elderly may be caused by aspiration due to swallowing difficulty.
- The eyes should be assessed for pupil size, equality, and reactivity to light and for the normal pink moist conjunctiva. The absence of yellowness of the sclera is important to rule out biliary obstruction, cirrhosis, or hepatitis.
Blood in the anterior chamber of the eye is called "hyphema" and indicates trauma--important for suspicion of child abuse.
- The ears should be assessed for pain and drainage.
Bleeding from within the ear post-traumatic mechanisms has a high likelihood of indicating a basilar skull fracture.
- The nose should be assessed for pain and nasal flaring. Nasal flaring indicates air hunger or hypoxia.
- The mouth should be assessed for foreign bodies, loose dentures, and for the normal finding of pink and moist mucosa. Tooth decay can overlay an abscess or indicate methamphetamine or cocaine abuse.
NECK: The neck should be assessed for pain, accessory muscle use, jugular vein distention, medical jewelry, and the presence of a stoma (current or previous tracheostomy).
CHEST: The chest should be assessed for
- shape,
- pain,
- equal rise and fall,
- breath sounds/noises,
- retractions,
- scars,
- medication patches, and
- medical devices. (Pacemakers.)
ABDOMEN: The abdomen should be assessed for
- pain,
- bowel sounds,
- rigidity,
- guarding,
- distension,
- scars,
- medication patches, and
- medical devices. (Intrathecal pain pumps are often placed in the anterior abdominal wall below and to one side of the navel.)
PELVIS: The pelvis and genitalia should be assessed for pain and incontinence.
EXTREMITIES:
The arms should be assessed for
pain,
distal circulation,
sensation,
motor function,
track marks, and
medical jewelry.
Petechiae and ecchymoses should be identified.
The legs should be assessed for
pain,
distal circulation,
sensation,
motor function,
track marks, and
medical jewelry.
Pain on walking or to squeezing the calf muscles can indicate deep vein thrombosis or thrombophlebitis.
BACK: The back should be assessed for pain, wounds, and scars.
Look and listen: just sizing up the general picture of how a person presents can be revealing--noting the things that are immediately noticeable. It only takes a moment.
Stroke
CRANIAL NERVES
A quick run-through of the Cranial Nerves (CN) for pertinent signs can often diagnose stroke and provide valuable information for the receiving neurologist. 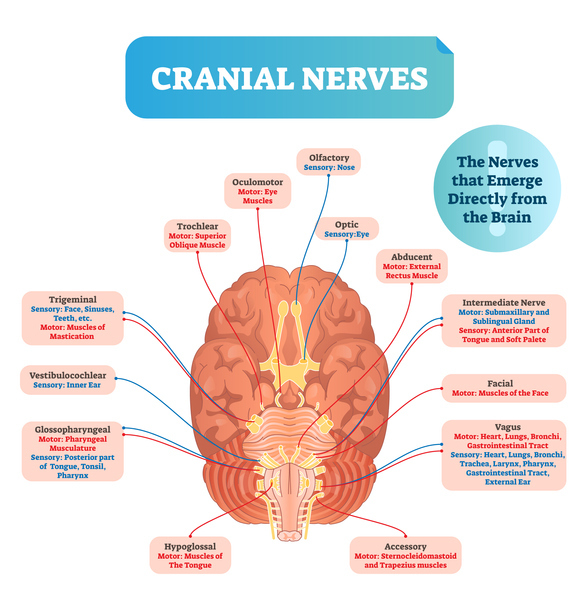
CN I: Smell. Generally not done.
CN II: deficits can be identified by gaps in the patient's field of vision and by abnormalities in the pupillary response to light.
Pupillary response to light is mediated by CNs II and III.
CN III, IV, VI: in strokes, paralysis of extraocular eye muscles may deviate the gaze (Cranial Nerves III, IV, VI).
CN V: Chewing and touch sensation on the forehead.
In unresponsive patients, the corneal reflex will document an intact CN V. (Touching the cornea with a cotton swab and eliciting a blink.)
CN VII: Fine facial expressions.
A good test is observing for balanced wrinkling of the forehead.
CN VIII: Balance.
Nystagmus is a positive finding for balance abnormalities.
CN IX and X: Swallowing, speaking.
Observe for balanced both sides of the palate when saying, "Aaah."
CN XI: Head movements.
CN XII: Tongue movements, speaking.
Evaluation of the tongue--see if it deviates when asking the patient to stick it out.
SOME PEARLS
Dysarthria means the impaired motor functions for speech, seen in abnormalities of CN IX, X, and XII.
Doll's eyes response: malfunction of one of the "gaze centers" (cortical and brain stem regions responsible for tracking by the eyes); when moving the head to one side, the eyes don't stay fixed but move with the head.
Barrel-chest: indicates increased AP chest diameter, as seen in emphysema.
Blood or CSF from the ear: indicates a basilar skull fracture.