Test Complete
- Questions
- Score
- Minutes
| Overall Results | |
|---|---|
| Total Questions |
| Category Results | |
|---|---|
Pressure Ulcers
Category: Special Populations
Topic: Geriatrics
Level: EMT
Next Unit: Pulmonary Considerations in the Elderly
14 minute read
DECUBITUS ULCERS: pressure ulcers that result in decay of body tissue due to pressure on a site.
Compression of soft tissue against a bony prominence collapses the vascular supply to that tissue, and unrelieved pressure, and thereby, ischemia, will cause necrosis.
Technically, pressure ulcers in this lesson are what are officially called "pressure-induced skin and soft tissue injury" to encompass the broad range of ischemic damage from prolonged pressure.
► While there can be superficial damage (lesser damage) that will not result in ulceration, it is important to know that deep tissue injury can occur without overlying skin ulceration.
Epidemiology
Pressure injuries are common among patients admitted to nursing homes, receiving home nursing, and in prolonged hospitalizations and long-term facilities.
Pathology
- Pressure applied to the skin in excess of arteriolar pressure (32 mmHg) prevents delivery of oxygen and nutrients to tissues, causing hypoxia and accumulation of metabolic wastes.
- Pressure applied to the skin in excess of 70 mmHg for two hours results in irreversible tissue damage, and ulcer formation may occur more rapidly with higher pressures.
Tissues vary in their susceptibility to pressure-induced injury:
- muscle is the most susceptible, followed by
- subcutaneous fat and then
- dermis.
Thus, extensive deep tissue damage can occur with initially little or no evidence of superficial tissue injury, although a deep tissue injury may then progress to the surface.
INFECTIONS: First colonized with skin flora, these are rapidly replaced by bacteria from the local environment and the urogenital or gastrointestinal tracts, often from direct fecal contamination. If infected, bacteria inhibit normal wound healing and promote further infection.
Cellulitis is a common bacterial infection of the skin and the underlying tissues, frequently caused by bacteria such as Streptococcus and Staphylococcus entering through breaks in the skin, including pressure ulcers. It often presents with symptoms like redness, swelling, warmth, tenderness, and purulent discharge, along with systemic signs such as fever, chills, and increased heart rate. In elderly, immobile patients with deep sores or pressure ulcers, cellulitis is a common and serious complication that can lead to sepsis, characterized by fever, tachycardia, and hypotension.
Risks
Risk factors vary according to the amount of pressure exerted and the duration of compression to the tissues. Also, an individual's susceptibility adds to the risk. The most important risk factors are:
- Immobility.
- Malnutrition.
- Reduced perfusion.
- Sensory loss.
Other considerations include fecal or urinary incontinence.
Adding the microbial pathogens from feces or the dampness of urine exacerbates the entire pressure ulceration process, making ulcerations beds of infection that can easily progress to the bony points that cause the pressure, resulting in osteomyelitis.
IMMOBILITY: Immobility (permanent or transient) is the most important host factor. Acute illness that makes mobility difficult or injury that makes it impossible to create immobility conditions that encourage the development of pressure ulcers.
MALNUTRITION: Tissue that is sub-optimized due to nutritional deficiencies will affect the severity of the injury, demonstrating a decrease in resiliency to hypoxia.
HYPOPERFUSION: It has been found that when vital organs such as the kidneys and the gastrointestinal tract are not adequately perfused, blood flow to the skin is also decreased, increasing the risk of pressure damage. Thus, atherosclerotic peripheral artery disease may precipitate ulcers because of baseline tissue hypoxia or a failure of blood flow to increase in response to pressure.
SENSORY LOSS: Pain acts as a warning signal that protects the body from harm. However, conditions like dementia, delirium, spinal cord injury, neuropathy, various neurological diseases, and diabetes often cause sensory loss. This loss dulls the ability to feel pain or discomfort from prolonged pressure, preventing individuals from taking action to relieve it. In particular, diabetic peripheral neuropathy numbs the feet to injury, allowing damage to go unnoticed and leading to the development of diabetic foot ulcers.
When you're sleeping, if you have undue pressure that interrupts blood flow, such as to a limb, you experience nociception (pain), which may be aching in nature or pins-and-needles. Even in your non-conscious state, you change positions and the pain resolves even before you wake up from it.
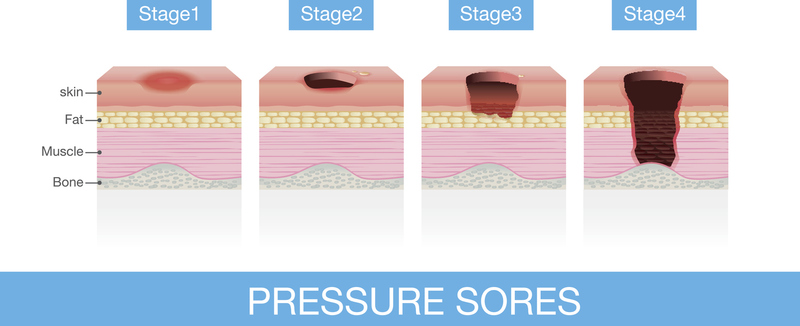
Clinical Staging
Stage 1: intact skin with a localized area of non-blanchable erythema.
Deep tissue pressure injury should be suspected whenever there is a localized area of skin (intact or non-intact) with persistent non-blanchable deep red, maroon, or purple discoloration or epidermal separation revealing a dark wound bed or blood-filled blister.
Pain and temperature change often precede skin color changes.
Stage 2: partial-thickness loss of skin with exposed dermis.
Stage 3: full-thickness loss of skin, in which fat is visible in the ulcer and granulation tissue and rolled wound edges are often present.
Stage 4: full-thickness skin and tissue loss with exposed or directly palpable fascia, muscle, tendon, ligament, cartilage, or bone.
Areas of Concern
Prolonged Supine Position:
- head,
- shoulder,
- back,
- hip,
- tailbone, and
- heel.
Prolonged Prone Position:
- head,
- jaw,
- elbow,
- breastbone (sternum),
- hip,
- knee, and
- shin.
Prolonged Lateral Position:
- shoulder,
- ribs,
- hip,
- knee, and
- ankle.
Management
Besides wound management, according to general principles of wound care, positioning the patient in alternating positions every 2 hours has been the classic approach, although results with scrupulous positioning schedules have been disappointing.
Today, great progress has been achieved with newer technology in hospital beds, such as air-fluidized mattresses and low-air-loss beds.
In the Field
In the field, your role in addressing pressure ulcers involves transporting the patient to a facility equipped to provide appropriate treatment.
Tissue damage and infection require time-consuming protocols that are not part of your obligations. However, if this is part of a larger picture of abuse or elder neglect, it is incumbent on you to report it.
Transport and support for other co-conditions (such as sepsis) with ABC (airway, breathing, and circulation), pain management, and other management at the BLS level are indicated.