Test Complete
- Questions
- Score
- Minutes
| Overall Results | |
|---|---|
| Total Questions |
| Category Results | |
|---|---|
Pediatric Assessment
Category: Special Populations
Topic: Pediatrics
Level: EMR
Next Unit: Abuse and Neglect
17 minute read
The Pediatric Assessment

This section will review some of the key considerations that must be made in the emergency evaluation of pediatric patients. Thought must be given to the environment the child was found in, their relationship with the parents, and their response to EMS personnel. This section will finish with an overview of the Pediatric Assessment Triangle (PAT) a structure rapid examination to asses the severity of an injury in a pediatric or non-verbal patient.
Scene safety
As with all patient encounters, you must begin with ensuring the scene is safe, perform a brief visual sweep of the area to ensure that there are no ongoing situations that could result in further harm patients, bystanders, or your team.
In calls involving pediatric patients, it is often helpful to search the scene for clues related to the chief complaint, many times items may be present that are a danger to a child but not an adult. Look for any pills, medicine bottles, chemicals, drugs, damaged electrical outlets, exposed cords, etc. If an animal that may have harmed the child is present, it should always be detained for examination. If this is required, a call to animal control is often the safest choice.
Special considerations
To a small child, the mere entrance of emergency responders can be intimidating. Minimizing potentially alarming lights, sirens, loud communication devices, and the number of providers near the patient will be beneficial to your examination. Many components of the initial evaluation can be done from a distance while speaking to one parent or another caregiver. When the examination requires patient contact involving parents or caregivers in any way possible will be helpful in keeping the child calm.
Always explain to children what you are doing, preparing them for what will happen (e.g., a brief pain in drawing blood, injections, or starting an IV), and use language they can understand.
Always pay attention to injury patterns in young patients. If injuries or behaviors are present that are suspicious for abuse, note your concerns and relay them to the appropriate authorities after the patient is stabilized. Do not challenge parents or bystanders on the scene in any circumstance.
The Pediatric Assessment Triangle (PAT)
The Pediatric Assessment Triangle (PAT) is a 15-30 second assessment of the severity of the patient's illness or injury. You can use this from across the room before beginning the proper ABCs and head-to-toe assessment. The pediatric assessment triangle has 3 parts, which can be remembered by the common acronym "ABC's"
- Appearance
- Breathing (work of breathing)
- Circulatory status
While this appears similar to the ABC's of stabilizing an emergency patient, the ABC's of the PAT is focused on the initial assessment of the patient, not the management of their condition. The PAT is most useful in ensuring that signs of an unstable pediatric patient are not missed.
Appearance
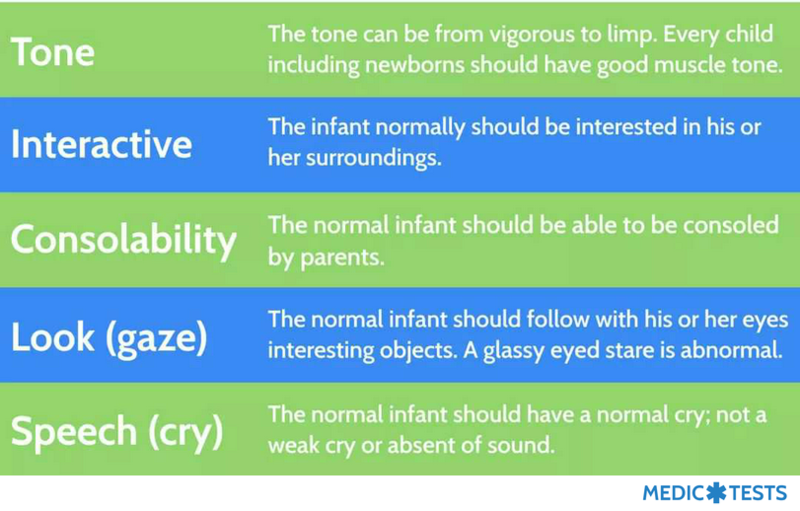
consists of evaluating the appearance of the child, including things like muscle tone, interactiveness, consolability, eye contact, and whether or not they are making vocalizations appropriate for their age. Younger children are often agitated, crying, and resistant to examination; this can make it challenging to distinguish between children who are appropriately distressed and those who are secondary to critical illness. For this reason, the mnemonic TICLS "Tickles" was created to assist with the assessment of a child's appearance.
It is also appropriate to use the AVPU scale in children to assess their overall level of consciousness. The scale is included here for review.
"Alert"?
Responsive to Verbal stimuli?
Responsive to Painful stimuli?
Unresponsive?
Work of Breathing
The work of breathing is a general assessment of the effort a child needs to put into taking a breath. The use of the neck muscles, retraction of the intercostals, flaring of the nostrils, and leaning over into a "tripod position" are all signs that work of breathing is increased. During the physical exam, lung sounds such as wheezing, stridor, and grunting may also point to increased work of breathing. (Grunting is accomplished via exhaling against a partially closed glottis, an intuitive action meant to keep the lower airway open.)
Circulatory Status
Observations that can clue you into a pediatric patient's circulatory status are the appearance of the skin. Skin that is cool to the touch, extremely warm to the touch, mottled, cyanotic, or covered in blood can all indicate different circulatory problems. Ensure that after the PAT rapid assessment you carefully check for signs of shock, with attention paid to the pulse quality in all limbs and the heart rate/sounds.
Other Elements of the Pediatric Assessment
An accurate history is vital in pediatric patients. Always attempt to ask the child first, especially if there was trauma leading to your call. This may not be possible or reliable, and even though clues from a physical exam may be difficult to acquire secondary to low patient cooperation, also utilize any available parents or guardians when gathering information. Ask about the onset and duration of symptoms, the child's recent activity levels, recent intake and output of food and waste, and a history of any vomiting, diarrhea, or abdominal pain.
Specifically, ask about any chronic illnesses, medical problems, or surgeries and any medications the patient is on or allergies they may have.
Head-to-Toe Exam
As in adults the head-to-toe exam or toe-to-head depending on the age, comes after the initial assessment and the assessment of the ABC's this exam is designed to unearth any life threats that may have been hidden during the initial examination, this section will list some of the pediatrics specific concerns to address in the head to toe exam.
- Fontanelles in infants can be used to gauge dehydration, albeit for a limited time. Sunken fontanelles indicated dehydration. Increased ICP and meningitis will cause bulging fontanelles.
The posterior fontanelle is usually closed by 2 months; the anterior fontanelle takes longer, generally sometime in the second year.
- Drainage of blood coming from the ears can suggest anything from a minor ear infection to a serious skull fracture.
- Blood in the pupil of the eyes is a sign of serious physical trauma, almost universally from abuse.
- Check the whole body surface for bruises, rashes, or injury. Be suspicious of bruises in children too young to crawl and bruises in strange areas such as the back of the arms, on the chest, and the hips, as these may be signs of abuse.
- Palpate the rib cage and be wary of areas of extreme tenderness, which may indicate rib fracture.
- Note whether the patient can move all extremities equally, this takes the place of a formal neuro exam in young children.
- In smaller children, take care to keep them covered whenever possible to prevent hypothermia.