Test Complete
- Questions
- Score
- Minutes
| Overall Results | |
|---|---|
| Total Questions |
| Category Results | |
|---|---|
Multi-quadrant Abdominal Pain
Abdominal Pain that Doesn't Fit Tidily or Exclusively into a Single Abdominal Quadrant
Most people call for help for one of three reasons:
- when something is painful;
- when something is bleeding; and
- when something isn't working properly, with bad events to follow.
These three reasons can be isolated, blended, or even dominoes falling in a sequence from one to the other. Because of this, there are conditions that will be encountered in the field which do not fit exclusively into one of the four quadrants of the abdomen. This can make diagnosis difficult.
IN THE FIELD: your role, thankfully, isn't necessarily to make the diagnosis, but to come up with a differential diagnosis--a list of possibilities THAT WILL ACCURATELY TRIAGE YOUR PATIENT.
As an EMS responder, you can then stabilize and--when indicated according to EMS criteria--transport the person to a facility appropriate for further diagnosis clarification. An exact diagnosis is THEIR job; YOUR job is to get them there.
Peritonitis
PERITONITIS: this is inflammation of the peritoneum, which can only happen if there is a diffuse infection or bleeding--from spillage of infectious material or internal bleeding, respectively. This is a surgical life-threatening emergency, so any rebound tenderness or diffuse pain throughout the abdomen requires immediate transport.
Pelvic Adhesive Disease (PAD)
PELVIC ADHESIVE DISEASE (PAD): this is a syndrome in which structures normally meant to be separate are adhered together due to previous surgery (most common), infection, scarring, or bleeding; the inflammatory process that created PAD was intended to seal the damaging inflammation from the rest of the body.
ADHESIONS: There is a curtain of fat extending from the bowel called the omentum. The omentum is quaintly called, by surgeons, "the abdomen's policeman." This is because it is the tissue that is naturally attracted to areas of inflammation in the abdomen and then attempts to wall these areas off, much like white blood cells and plasma immune cells wall off infections in the skin (abscess)--the abscess wall being that dividing structure between the person and the infection being. This quarantine of sorts is, therefore, a protective mechanism to keep the bad stuff away from the good stuff. However, after the inflammation has resolved, the omentum remains stuck to the spot it was "policing." This is called an "adhesion," and it can remain there lifelong.
From beginning to end, the bowel is meant to be free floating in the abdomen, so if there are adhesions, there could be immobilized sections of the bowel that are immoveable kinks in the path for feces to travel; this causes distension at the kinks during transit. Since the peritoneum responds painfully to distension, adhesional pain can present anywhere in the abdomen where adhesions are. It is
- sharp,
- colicky, and
- usually temporary.
Occasionally, a stretch of bowel may become so kinked that feces cannot make it past the challenging area, and an acute obstruction occurs, which is a surgical emergency.
Pelvic adhesive disease is most commonly seen at sites of previous surgery (internal scarring) or areas previously affected by infection or hemorrhage, but they can also involve most--even all--of the GI tract to cause pain in any and all quadrants.
CAVEAT: It is clinically impossible to distinguish between partial obstruction (not a surgical emergency) and complete obstruction (which is), so transport is the default position.
Inflammatory Bowel Disease (IBD)
INFLAMMATORY BOWEL DISEASE (IBD) includes irritable bowel syndromes (IBS) and immunological inflammatory diseases such as Crohn's disease and ulcerative colitis. These are dealt with specifically in another unit [SEE "INFLAMMATORY BOWEL DISEASE."] The point to be made here is that with over 20 feet of the small bowel and 5 feet of the large bowel tends to be all over the abdomen, and pain from it can occur anywhere and in combinations of locations throughout the abdomen.
Urinary Tract Problems
BLADDER SPASM AND URINARY TRACT INFECTIONS: these usually create pain in the mid-lower abdomen and the medial portions of the LLQ and RLQ. If the urinary infection ascends higher than the bladder--into the kidney(s)--there can be an exquisitely sensitive back pain at the mid-back. The back pain, as is seen with a kidney infection (pyelonephritis) can be unilateral (left or right mid-back) or bilateral.
NEPHROLITHIASIS (Kidney Stone): a stone--either lodged (immobile) or migrating down the ureter--will cause sudden, sharp, excruciating pain in either flank and the upper LLQ or RLQ, depending on which kidney or ureter--R or L--is involved; stones are usually accompanied by bloody urine.
The pain is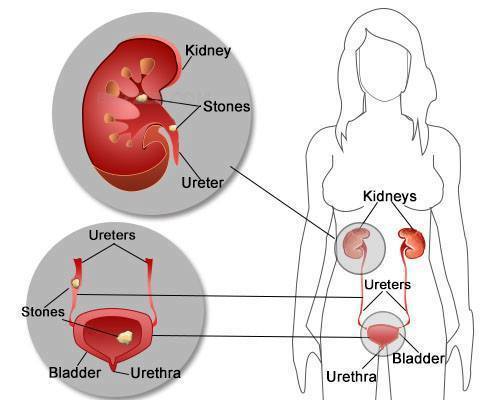
- flank pain and
- migrates downward with the mobility of the stone down the ureter. It is a
- very sharp, completely debilitating pain
that requires transport, at the very least, for acute pain management.
KIDNEY OBSTRUCTION, INFECTION, OR STONES: such kidney conditions present with unilateral pain (sometimes bilateral if both kidneys are involved). This pain is posterior, elicited easily by the patient's negative reaction to a light tapping on the mid-back area on either or both sides. Being retroperitoneal, the kidneys don't often figure into dramatic presentations of anterior abdominal pain, although migrating stones can cause pain anywhere along their journey (RUQ → RLQ or, alternately; LUQ → LLQ).
Bowel Disease
BOWEL OBSTRUCTION: when the intestines become partially or completely blocked, the contents pile up and result in abdominal swelling and pain above the obstruction. The pain can present wherever the obstruction distends the bowel (and above), which can involve more than one quadrant. Vomiting is common; in severe cases, patients may vomit fecal matter.
Other causes of obstruction of the upper GI tract can cross quadrant lines:
- PYLORIC STENOSIS, actually not in the bowel, but in the stomach, can cause pain in the LUQ and somewhat radiate over the midline toward the right. It is included here because it will be impossible for you to tell where the obstruction is.
- INTESTINAL OBSTRUCTION lower than pyloric stenosis is typically in the RLQ and/or LLQ, since the bowel occupies both quadrants.
- INCARCERATED UMBILICAL HERNIA, however, can result in central abdominal pain AND pain referred to that part of the abdomen responsible for nerve sensation to the respective portion of the bowel that is incarcerated.
INCARCERATED HERNIA: a hernia is a separation or widening of an opening in the tough fascia (main constraining layer of the abdominal wall). The inguinal and umbilical areas are natural weakness points. Previous surgery scars are acquired weakness points. If one of these areas widens enough, the bowel can poke through it and then not be able to fall back in, trapping it in serious jeopardy of obstruction and even ischemia and tissue death.
- INGUINAL HERNIA: depending on whether right, left, or bilateral, inguinal hernia will present as pain in the RLQ, LLQ, or both, respectively. Incarceration, in which bowel contents become trapped, will raise the level of pain considerably due to obstruction and possibly even bowel death. Telltale bulge(s) can be seen and voluntary guarding is usually present. Any suspected incarceration of the bowel, anywhere, is a time-sensitive urgency to transport.
- UMBILICAL HERNIA: any umbilical hernia in the central abdomen, likewise, can cause incarceration of the bowel, and the pain can be referred to the quadrant in which that portion of the trapped bowel normally resides. Therefore, if a portion of the ileum gets trapped, the pain can be reported as coming from the RLQ, even though the origin of the pain is from the area of entrapment--the midline umbilicus.
Reduction of Incarcerated Hernia: because of the mechanical nature of hernias, temporarily incarcerated hernias of entrapped bowel can usually be gently "milked" back through the opening that allows them to protrude in the first place if your local protocols allow. This can be done in the field and, with successful replacement of the bowel, the symptoms will dramatically improve, possibly sparing the person transport. However, like anything in medicine, nothing should be forced.
►Call to Action: TRANSPORT
Any failed attempt at GENTLY pushing the bowel back through should prompt immediate transport. Any continued pain, even after replacement (reduction of a hernia), should make you suspect ischemia and/or infarction of the tissues that were trapped (= immediate transport).
Female Reproductive Organ Problems
OVARIAN CYST: can present as a sharp pain on one side (unilateral) or both sides (bilateral), but usually unilateral. If the sharp pinpoint pain suddenly converts to a vague, diffuse burning sensation across the entire pelvis, this indicates rupture of an ovarian cyst with limited bleeding into the abdomen (or abscess, with pus from rupture).
"MITTELSCHMERTZ": from the German, "middle pain," referring to the mid-cycle sensation of ovulation in some women able to discern it: it is the pain of ovulation.
►Call to Action: TRANSPORT
Because an ectopic pregnancy is always in the differential diagnosis, ovarian cyst, cyst rupture, or--Achtung!--even Mittleschmertz will require transport as a precautionary measure, even if the vitals are stable.
UTERINE PAIN: endometritis (infection of the uterus, or womb) is usually a part of the salpingitis seen in STDs and will present as midline, lower pelvic pain, frequently accompanied by a fever. With accompanying salpingitis, the entire LLQ, RLQ--or both--can be involved.
NOTE: Toxic Shock Syndrome can begin like this, which like endometritis, can be accompanied by high fevers and both require transport to prevent or address sepsis.
PELVIC FLOOR SPASM: any type of pain in the pelvis/abdomen can cause a reflexive contracting of the pelvic floor musculature to splint pain away, resulting in pelvic floor overuse, strain, and/or spasm which can remain even after the original source of pain resolves. Pelvic floor spasms can refer to pain to the LLQ and RLQ of the female abdominal wall, which results in considerable confusion as to the original cause.
ENDOMETRIOSIS: menstrual-like tissue that is lodged in the pelvis, causing cyclic inflammatory reactions of the peritoneum. Its presence can range from a single implant to widespread dissemination throughout the pelvis: its pain can be pin-point or diffuse and can cross to different abdominal quadrants. The monthly appearance of the same symptoms suggests the diagnosis.
Pancreatic Disease
PANCREATITIS is an inflammation of the pancreas. It can be acute or chronic and is caused primarily by gallstones or heavy alcohol use. Also, malignancy can obstruct the pancreatic duct resulting in severe, sudden pain. Abdominal pain associated with pancreatitis is primarily
- in the upper half of the abdomen,
- radiating to the back, and
- gets worse after eating (when digestive enzymes are released). Also,
- vomiting,
- fever, and
- tachycardia can also be symptoms of pancreatitis.
Pancreatitis usually is not life-threatening but can lead to infection and sepsis.
Lung Disease Referring Symptoms to the Abdomen
PLEURISY (PLEURITIS): an inflammation of the lining of the lungs. It can also involve the areas adjacent to the diaphragm. As such, pain syndromes can present which mimic RUQ (liver, gallbladder) or LUQ (spleen), with referred pain to the right or left shoulder/shoulder blade, respectively. This confusion can only be sorted out by transport to an adequate diagnostic facility. The pain is
- sharp,
- knife-like, and
- peaks with each breath, coughing, or sneezing.
People with COPD may have worsening compromise due to the splinting of their intercostal muscles to limit the volume of air inspired (and the amount of distention with each inspiration) that stretches the pleura, all in an attempt to splint the pain from lung expansion. COPD sufferers certainly don't need any more restrictions on their ventilation!