Test Complete
- Questions
- Score
- Minutes
| Overall Results | |
|---|---|
| Total Questions |
| Category Results | |
|---|---|
Influenza
Category: Medical
Topic: Infectious Diseases
Level: Paramedic
Next Unit: Mononucleosis
12 minute read
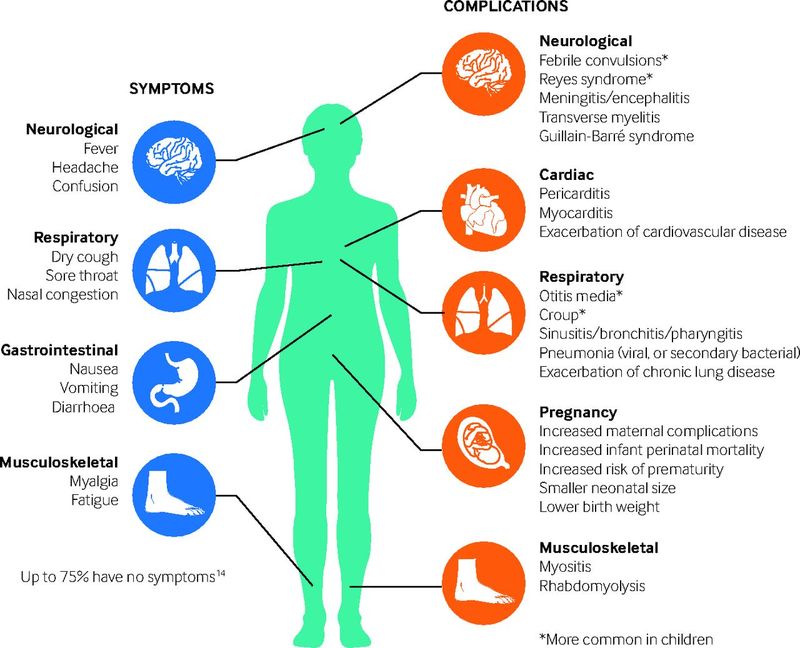
Definitions and Epidemiology
Influenza, commonly known as the “flu,” is a seasonal infectious disease that causes
- fever,
- runny nose,
- sore throat,
- muscle pains,
- headache,
- coughing, and
- fatigue.
INFLUENZA A and INFLUENZA B:
Acute respiratory illness caused by influenza A or B viruses occur in outbreaks and epidemics worldwide, mainly during the winter season.
INFLUENZA C has been reported to cause acute respiratory illnesses in children and, more rarely, in adults.
MUTATION: Influenza A viruses, especially, can change the antigenic characteristics of their envelope proteins--the hemagglutinin and neuraminidase ("H" and "N"). There are three different subtypes of "H":
- H1,
- H2, and
- H3;
and two subtypes of "N":
- N1 and
- N2.
The hemagglutinin (the "H" of H/N) is what sticks to epithelial cell surface proteins, necessary for infection.
Antigenic Shifts
Major changes in the envelope proteins, H and N, are called antigenic shifts, and minor changes are called antigenic drifts.
Antigenic shifts are associated with epidemics and pandemics of influenza A, whereas antigenic drifts are associated with more localized outbreaks of varying extent.
The pandemic of 1918 involved shifts in both H1 and N1 of influenza A. Today, the H1N1 is called swine flu. Other variants can see the proteins jumbled as H3N2, H2N2, etc. This makes a universal vaccine impossible.
Transmission
Large amounts of influenza virus are often present in respiratory secretions of infected persons, so infections are transmitted through sneezing and coughing via both large droplets (>5 microns) and small particle aerosols. Acquisition via large-particle droplets requires close contact, since large particles do not remain suspended in the air and travel only short distances (approximately 6 feet), while small particle aerosols may travel for longer distances.
Influenza, besides spreading by airborne means, is also spread when in direct contact with saliva or mucosal fluids from infected persons, and with indirect contact with surfaces that have infected material on them.
►Soap renders the virus inactivated, so hand-washing is the best preventive practice.
Signs and Symptoms (S&S)
INCUBATION PERIOD: 1-4 days (usually 2).
INFECTIOUS PERIOD: Viral shedding is from 1-2 days before symptoms and for about 5 days.
2 days < SYMPTOMS > 5 days
Shedding doesn't generally occur after 6 days. Longer periods of shedding can occur in children, the elderly, and the immunocompromised. The magnitude of shedding correlates with the severity of illness.
SYMPTOMS: Symptoms usually begin two days after initial exposure to the virus and most last less than a week. A cough, however, may last for more than two weeks. (Children may present with nausea and vomiting, but this finding is not common in adults.)
GENERAL ASSESSMENT FINDINGS:
- upper respiratory illness-type symptoms,
- a cough that is often severe and protracted,
- fever, and
- body aches.
High-Risk Populations
- Residents of nursing homes and long care facilities.
- Age 65 years and older.
- Pregnant women and recently delivered women.
- Pulmonary disease (including asthma, COPD, emphysema).
- Cardiovascular disease.
- Active malignancy.
- Renal disease.
- Liver disease. ? Diabetes.
- Blood disease, such as sickle cell anemia.
- Immunosuppression (HIV+, transplant patients).
- Those on immunosuppression for autoimmune diseases (rheumatoid arthritis, psoriasis, etc.).
- Neurologic conditions that interfere with handling respiratory secretions (stroke patients, closed brain injuries).
- Morbidly obese.
- Native Americans and Alaskans.
Complications
Complications common to persons infected with influenza include:
- viral pneumonia,
- bacterial pneumonia,
- sinus infections and sinus headaches, and
- worsening of previous health problems such as asthma or heart failure.
Prevention
- Hand hygiene and face masks.
- Vaccination (applies to specific strains and is dependent on predictive accuracy).
Recommended: vaccination for everyone older than 6 months, with high-risk populations and healthcare workers being a high priority.
Management
Treatment is selectively chosen for high-risk groups, those requiring hospitalization, or those with progressive illness.
Adults with mild illness without high-risk conditions who are younger than 65 years of age do not require testing or treatment. Otherwise, when indicated,
- antiviral therapy for the primary disease, and/or antibiotics for secondary bacterial infection complications, pneumonia, otitis media, or sinusitis.
- Acetaminophen or NSAIDs can be used for fever, headache, and myalgia. Aspirin (and salicylates) should be avoided because of the risk of Reye syndrome, especially the young.
In the field, general management for a patient with influenza is supportive and includes
- isolation procedures for the providers as well as
- maintaining ABC (a patent airway, ensuring and assisting adequate respiration, oxygenation and ventilation, circulatory support),
- IV fluids if dehydrated,
- pain management, and
- transport to definitive care.
Post-exposure considerations include
- general wellness checks and
- follow-up with infectious exposure personnel and vaccination.