Test Complete
- Questions
- Score
- Minutes
| Overall Results | |
|---|---|
| Total Questions |
| Category Results | |
|---|---|
Inflammatory Bowel Disease
Category: Medical
Topic: Abdominal and Gastrointestinal Disorders
Level: EMT
Next Unit: Common Abdominal Pathologies
19 minute read
Inflammatory Bowel Disease (IBD) vs Irritable Bowel Syndrome (IBS)
First things first, a word about Irritable Bowel Syndrome:
Irritable Bowel Syndrome (IBS) is NOT Inflammatory Bowel Disease (IBD), discussed here.
This unit is about Inflammatory Bowel Disease, whereas Irritable Bowel Syndrome (IBS) is a common and vague disorder that affects the large intestine, resulting in cramping, abdominal pain, bloating, gas, diarrhea, and constipation--a syndrome of symptoms. It is a chronic condition.
Irritable bowel syndrome may turn out to be inflammatory bowel disease once all the facts are in, but when referring to an alteration in bowel habits and abdominal pain WITHOUT a definable organic cause, the trashcan diagnosis of irritable bowel SYNDROME is used. That is, one is a disease, the other a syndrome, and they are labeled as such.
Inflammatory bowel disease (IBD): in contrast to the syndrome of IBS, the disease of IBD has clinical and laboratory (biopsy/endoscopy) evidence that determines its diagnosis.
In other words, irritable bowel syndrome is unofficial, while inflammatory bowel disease is official.
Inflammatory Bowel Disease
IBD usually refers to one of two major disorders:
- Ulcerative colitis (UC)
- Crohn disease (CD)
Both usually arise between ages 15 and 40, peaking between 50-80 years of age. They are both categorized together because while each is a distinct entity, they both have overlapping pathology and clinical presentations:
- Ulcerative Colitis: recurring episodes of inflammation limited to the internal (mucosal) layer of the colon. It is typically in the rectum but may extend by direct continuity into the higher parts of the large colon (descending, transverse colon).
- Crohn Disease: involves inflammation through the entire wall of the colon and can spread by skips instead of via a continuous spread.
Unlike UC, which is centered on the rectum, CD can involve any area from mouth to anus. Because the entire wall of the colon is involved, this can cause fibrosis and strictures, leading to obstruction, and sinus tracts that can cause "microperforations" and fistulas.
Since both conditions are a type of systemic autoimmune/inflammatory condition, both can also have inflammatory problems outside of the bowel:
- arthritis of the large joints, osteoporosis,
- eye inflammation (uveitis, conjunctivitis, etc.),
- skin problems such as erythema nodosum (nodular patches of red skin),
- liver changes, such as fatty liver,
- blood coagulation problems (coagulopathies), such as venous thromboembolism with flares, and/or
- acute hemolytic anemia.
Ulcerative Colitis
The usual presentation is
-
bloody diarrhea.
UC should be suspected if there is chronic diarrhea lasting longer than 4 weeks, although true UC typically has attacks of bloody diarrhea lasting weeks to months with periods of complete remission in between. Bowel movements (BMs) are small and frequent. There is colicky abdominal pain, the urge to defecate, and incontinence. The range of symptoms goes from 1-4 stools/day without blood to > 10 stools a day with severe cramps and continuous bleeding.
ACUTELY, there may be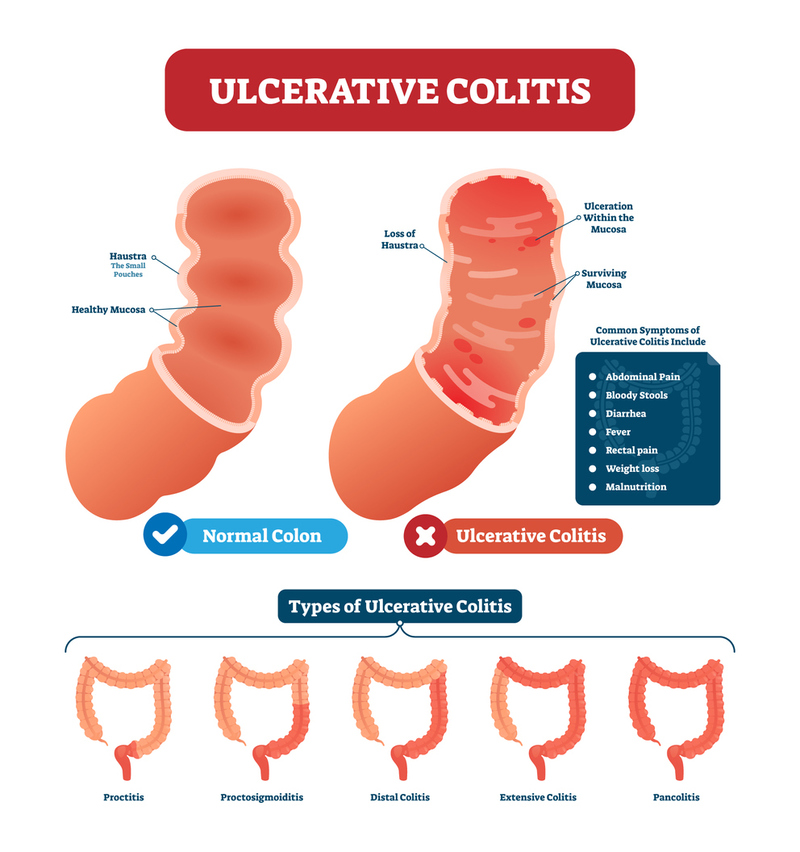
- prolonged diarrhea;
- fever;
- fatigue;
- weight loss;
- anemia: there may be severe enough anemia to cause difficulty breathing and palpitations, pallor, hypotension, and tachycardia;
- abdominal tenderness to palpation.
CHRONIC complications include
- strictures and
- colorectal cancer.
UC "wannabes": besides Crohn Disease (see below), a previously well person who develops unremitting diarrhea should be evaluated for Salmonella, Shigella, and other infectious colitis syndromes.
In the field, these cases won't have their final diagnosis until after transport, so your EMS responder concerns should revolve around dehydration, electrolyte disturbances, and hypovolemic blood loss.
CALL TO ACTION--TRANSPORT:
In the field, acute complications are related to severe bleeding and if the disease extends beyond the mucosal layer, perforation.
Severe anemia and hypovolemic shock require the ABCs maintenance (airway, breathing, and circulation).
Perforation will create a peritonitis with rebound tenderness, guarding, and a 50% mortality rate!
The longer a person has UC, the more likely acute complications will occur, so any person with a years-long history of UC, along with pallor, pain, hypotension, and signs of peritonitis, requires immediate transport.
Crohn's Disease
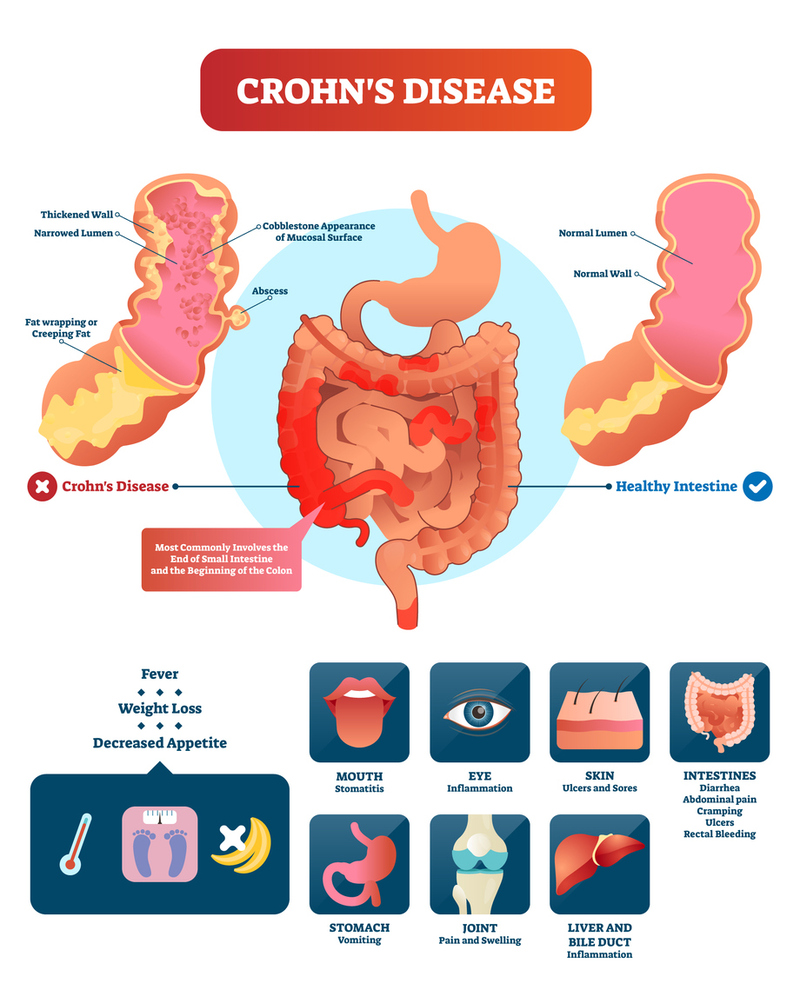
The usual presentation is
- prolonged diarrhea, with or without blood, accompanied with
- fatigue,
- weight loss,
- fever, and
- abdominal pain.
The abdominal pain results from the fibrosis of the colon wall that causes obstruction.
There is less frank blood than with UC. Bowel movements (BMs) may have blood, but the amount is generally less than that encountered with ulcerative colitis.
ACUTELY, there may be:
- prolonged diarrhea,
- fever,
- fatigue, and/or
- abdominal cramping.
CHRONIC COMPLICATIONS include
- fistulas,
- diarrhea,
- weight loss,
- strictures/obstruction,
- abdominal abscesses/peritonitis, and/or
- peri-anal disease.
- Fistulas (connections between two body areas) can form, most frequently between the intestines and the bladder--causing recurrent urinary tract infections due to seeding the sterile bladder with colonic bacteria; intestines to the skin--causing fecal drainage on the skin; intestines to the vagina--causing feces or flatus through the vagina and chronic vaginitis; and one part of the intestines to another part--usually without specific symptoms. Up to 1/2 of persons with CD will develop fistulas after 10-20 years of CD, some of them before the diagnosis is even made.
- 1/3 of CD patients have a peri-anal disease (anal pain, drainage, and abscess).
- Malabsorption: unabsorbed bile salts can cause "bile salt" diarrhea--watery diarrhea and steatorrhea (fat in the feces), resulting in malnutrition, Vitamin B12 deficiency, coagulopathy, and hypocalcemia/osteomalacia with kidney or gallstones.
Both UC and CD can result in perforation of the bowel: UC inflammation can spread to involve the muscular portion of the bowel wall, allowing distention ("megacolon") to the point of perforation, whereas CD can have perforation from the fistula process.
CALL TO ACTION--TRANSPORT:
In the field, acute complications are related to acute obstruction.
UC vs. CD
COMPARING AND CONTRASTING UC with CD--a CHEATSHEET
While the similarities between UC and CD include
- fatigue,
- pain,
- fever, and
- weight loss,
the differences between them are:
- Involvement of the colon wall:
UC involves the mucosal (innermost) layer of the colon wall;
CD involves all layers of the entire colon wall ("transmural").
- Extension of the disease:
UC usually involves the rectum first/foremost and spreads by direct extension into adjacent areas ("contiguous" spread);
CD can be anywhere from the mouth to anus, but it usually spares the rectum. CD also extends via a tendency to skip areas and appear according to a non-contiguous spread.
(UC reaches out locally, while CD skips considerable distances.)
- Diarrhea:
UC usually has diarrhea associated with gross blood, frequent and small BMs;
CD usually has diarrhea without gross blood, but if there is blood, it is less than with UC--usually microscopic.
- Specific site pain:
UC has rectal pain, but CD has peri-anal pain from peri-anal diseases such as abscesses, fissures, and fistulas.
- Strictures and obstruction:
UC causes strictures in 10%, leading to obstruction, but usually in the rectosigmoid colon;
CD causes strictures in over 50%, long-term with obstruction occurring anywhere.
- Perforation:
UC can have a perforation from "megacolon," a dilation of the bowel that occurs when the inflammatory process goes beyond the mucosa to involve the muscular later;
CD can result in perforations from fistula formation.
- Pain:
UC has colicky abdominal pain from inflammation;
CD has crampy abdominal pain from partial or complete obstructions.