Test Complete
- Questions
- Score
- Minutes
| Overall Results | |
|---|---|
| Total Questions |
| Category Results | |
|---|---|
EMT MANAGEMENT OF CHEST INJURY
Category: Trauma
Topic: Chest Trauma
Level: EMT
Next Unit: Blunt Cardiac Trauma and Commotio Cordis
31 minute read
Chest trauma can result in several injuries that may be fatal to a patient if they are not stabilized prior to transport. These injuries can be roughly divided into open and closed chest injuries, based on whether or not the chest cavity is exposed to the surrounding atmosphere. This section will discuss how these injuries relate to the ABCs and various life threats.
Closed Chest Injury
The key closed chest injuries are secondary puncture injury, flail chest, sternal fracture, and commotio cordis.
SECONDARY PUNCTURE INJURY: Fragments or sharp ends of fractured ribs can lead to the puncture and bleeding of organs within the chest and abdomen. Due to their proximity to the ribs, the most common organs involved are the lungs, liver, and spleen.
Puncture of the lungs can lead to pneumothorax, which will compromise breathing, and/or tension pneumothorax, which can compromise both breathing and circulation. Liver and Splenic puncture can lead to massive internal bleeding due to the extreme amount of blood that normally flows through these organs every minute.
For all forms of internal injury secondary to a rib fracture, surgery is necessary, making transport to a trauma center an urgent necessity. Patients suspected of having internal bleeding should be frequently re-assessed to determine if they require IV fluids or blood products.
FLAIL CHEST: A flail chest can occur when two or more ribs are broken in two or more places. Creating a floating island of the chest wall with no bony support that moves at a different rhythm from the rest of the chest. This "flail segment" causes extreme pain as the broken ends of the fractured ribs rub with each breath. When multiple adjoining ribs fracture, the chest wall can fully lose rigidity. This results in a larger flail segment that moves with the lungs instead of staying stationary, allowing proper lung expansion/contraction. This is termed "paradoxical movement."
Paradoxical movement of the chest results in significantly reduced ventilation, which leads to the symptoms of shortness of breath, difficulty breathing, and extreme pain. If untreated with positive pressure oxygen and rapid surgery, this will lead to low oxygen saturation and potential organ damage resulting from hypoxia.
Positive pressure ventilation is the definitive treatment as it removes the need for a rigid chest wall to draw air into the lungs. If positive pressure ventilation is unavailable or the patient cannot cooperate with ventilations given by bag-valve-mask, 100% oxygen may temporarily stabilize patients.
STERNAL FRACTURE: Rarely dangerous on its own, a fracture of the sternum commonly presents secondary to high-energy trauma, which damages the underlying lung/heart/vessels. Depending on which underlying structures are damaged, this can lead to airway, breathing, or circulatory compromise.
The most commonly injured organs in sternal fracture are the lungs, followed closely by the heart, spine, esophagus, trachea, and large blood vessels within the chest.
COMMOTIO CORDIS: An induced arrhythmia in the heart secondary to blunt force impact at specific times in the cardiac cycle.
This condition is more common in children and adolescents due to the greater flexibility of the sternum and ribs, allowing for more impact force to reach the heart. Even minor impacts can induce commotio cordis, meaning that obvious bruising, fractures, or other injuries may not exist. The history of a sudden collapse followed by instant unconsciousness and loss of pulse following an impact on the chest is the classic story of commotio cordis.
The loss of consciousness is due to compromised circulation due to cardiac arrhythmia. Patients with commotio cordis require CPR prior to EMS arrival and eventual defibrillation to survive. While the best results are obtained by following ACLS algorithms, using an AED will also prove beneficial.
OTHER CLOSED CHEST INJURIES: Many other closed chest injuries do not require special treatment in the EMS setting. Supporting the ABCs and arranging rapid transport is generally sufficient for these complications of trauma.
- Cardiac Contusion: Results from significant impacts to the chest can result in hypotension, myocardial infarction, or cardiogenic shock,
- Pulmonary Contusion: This can result from more minor impacts, generally presents with shortness of breath and pain, and may advance to severe respiratory compromise.
- Vessel Transection: Results from high-energy trauma and generally results in instant unconsciousness due to a massive and instantaneous drop in blood pressure.
- Spinal Fracture: This can result from any trauma to the chest, as the ribs connect to the spinal column. Generally requires high-energy trauma in healthy young individuals.
- Tension and bilateral pneumothoraces: All traumatic arrests with steering wheel damage get automatic bilateral needle decompression!
According to Emerg Med J. 2009 Oct;26(10):738-40, "Chest decompression in traumatic cardiac arrest identifies and treats a high proportion of potentially life-ending injuries and should be considered as part of the resuscitation effort of patients in traumatic cardiac arrest. In many patients, non-survivable injuries are identified which guide resuscitation efforts."
Open Chest Injury
The key open chest injuries are pneumothorax, open pneumothorax, hemothorax, and cardiac tamponade,
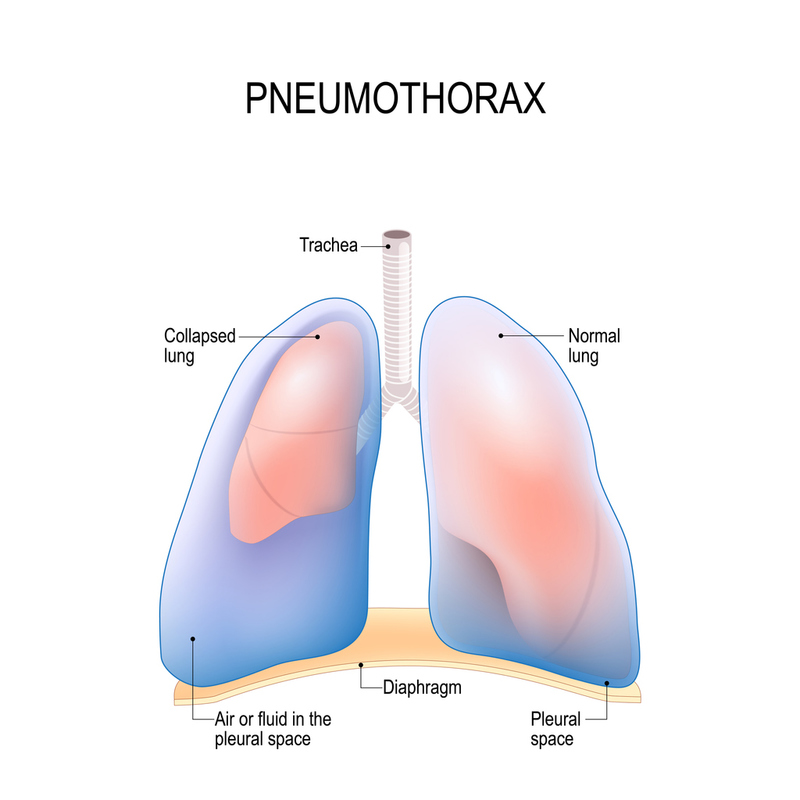
PNEUMOTHORAX: a collection of air in the chest cavity due to an internal lung structure rupture. While not open to the outside of the chest wall, they are often considered an open injury as they result from trauma to the inner lung, opening the chest cavity to the atmosphere through the bronchi/trachea.
A pneumothorax can occur due to trauma, causing the bronchi to tear or small collections of alveoli (blebs) to rupture, spilling air into the chest. If this air pocket expands far enough, it can prevent lung expansion by replacing the lung's space in the chest with air. In extreme cases, each patient's breath will draw more air into the chest, raising the pressure within the chest and resulting in a tension pneumothorax.
The signs and symptoms of a pneumothorax only become apparent when the lung is collapsed enough to limit oxygen exchange, the timeline over which this occurs is different for each patient. Younger and healthier patients generally take much longer to begin showing symptoms. Gradually increasing shortness of breath, lightheadedness, and altered state of consciousness are the most common symptoms of pneumothorax. A decrease in breath sounds over the affected lung is the earliest exam finding, and a decrease in oxygenation is the typical late exam finding.
In the case of a tension pneumothorax, deviation of the trachea away from the affected side and hypotension (due to cardiac compression) are seen. The treatment for pneumothorax is 100% oxygen via a non-rebreather mask. Avoid positive pressure ventilation if possible, as this may expand the pneumothorax or convert it into a tension pneumothorax. If you suspect a tension pneumothorax, needle decompression is required. Often, the pressure in the chest will rise fast enough that the patient will die in transport unless the pressure is released.
SPONTANEOUS PNEUMOTHORAX: This type occurs without an obvious cause or preceding trauma. It's often divided into primary and secondary types. Primary spontaneous pneumothorax occurs in people without underlying lung diseases and is believed to result from the rupture of small, air-filled blisters on the lung's surface (blebs). Secondary spontaneous pneumothorax is associated with existing lung conditions, such as chronic obstructive pulmonary disease (COPD), cystic fibrosis, or asthma, where the lung disease leads to the pneumothorax.
SIMPLE PNEUMOTHORAX: A simple pneumothorax is the presence of air in the pleural space without a significant shift of the mediastinal structures or hemodynamic instability. It typically results from the rupture of a small bleb or due to minor trauma. Unlike a tension pneumothorax, it does not feature the rapid accumulation of air under pressure that can lead to life-threatening changes.
The clinical presentation of a simple pneumothorax may include sudden onset of chest pain and mild to moderate dyspnea. Physical examination may reveal decreased breath sounds on the affected side without the presence of tracheal deviation or hypotension that characterizes tension pneumothorax.
Management of a simple pneumothorax in the prehospital setting focuses on monitoring and supporting the patient's respiratory function. Administration of supplemental oxygen is recommended to enhance the reabsorption of air from the pleural space. Transport to a healthcare facility for further evaluation and management is necessary. In cases where the pneumothorax is small, and the patient is stable, observation and supplemental oxygen may be all that is required. However, larger pneumothoraces or those causing significant symptoms may necessitate more aggressive interventions such as needle aspiration or chest tube placement.
OPEN PNEUMOTHORAX: An open pneumothorax results from an external wound allowing air into the chest cavity instead of the internal rupture of air-containing structures. Often called "sucking chest wounds" due to the gurgling sounds that are made when blood from the wound mixes with air that is being sucked into the chest cavity while breathing.
Open pneumothoraces are managed with specific dressings: three-way dressings, occlusive dressings, or chest seals. These prevent additional air from entering the wound upon inspiration while allowing air in the chest cavity to exit the wound as the patient moves and breathes naturally.
Besides the placement of a chest seal and monitoring bleeding, the management of an open pneumothorax is the same as a closed pneumothorax (oxygen, monitors, and frequent reassessment). Note that there is an elevated risk of these wounds converting to tension pneumothorax; be quick to perform a needle decompression in these patients if they deteriorate during transport.
HEMOTHORAX: Similar in effect to a pneumothorax, a hemothorax is the filling of the chest cavity with blood, which displaces the room the lung uses to expand. Decreasing the amount of air that can enter the lung tissue and exchange oxygen with the blood. It is important to remember that "hemothorax" refers specifically to the blood outside the lung tissue. "pulmonary hemorrhage" refers to blood within the lung, often both present together.
The management of hemothorax is largely identical to pneumothorax, with oxygenation and ventilation being the primary concerns for the patient. The major difference is the significant risk of hemorrhagic shock resulting from the loss of significant blood volume into the chest cavity, it is possible to lose enough blood volume internally in the chest cavity to cause death. Watch closely for the early signs of blood loss (headache, tachycardia, tachypnea) and be ready to provide circulatory support.
Patients with significant hemothorax almost universally require urgent surgery. Consider transporting these patients to a certified trauma center to facilitate treatment.
CARDIAC TAMPONADE: The filling of the space between the pericardium and the heart with blood or other fluid. Like a hemothorax, filling this normally empty space results in decreased space for the heart to expand and fill with blood between beats. The smaller size of the heart compared to the lungs means that a very small amount of fluid can lead to fatal hypotension secondary to reduced cardiac output.
Tamponade can occur in trauma (due to hemopericardium) but is more often the result of medical problems, kidney failure, liver failure, and cancer can all lead to fluid filling this space (known as pericardial effusion). The telltale symptoms of tamponade are known as "becks triad," Hypotension, distant heart sounds, and distention of the neck veins. Management is based on providing 100% oxygen to maximize the effect of the little blood that the heart can still pump while transporting the patient to a trauma center for urgent surgery.
Paramedics or AEMTs can perform lifesaving "pericardiocentesis" (needle drainage of the pericardium) in some jurisdictions. This procedure requires specific training and permission from the medical command.