Test Complete
- Questions
- Score
- Minutes
| Overall Results | |
|---|---|
| Total Questions |
| Category Results | |
|---|---|
EMT Considerations in Orthopedic Trauma
Category: Trauma
Topic: Orthopedic Trauma
Level: EMT
Next Unit: Basics of Orthopedic Trauma
28 minute read
Joint Anatomy
Joints are structures where two parts of the skeleton fit together (articulate.) They are padded by cartilage, a pliable tissue that also forms structures like the ear and nose.
The major types of joints are
- Synovial
- Gliding
- Hinge
- Ball & Socket
SYNOVIAL JOINTS are enclosed by protective sacks filled with synovial fluid which keeps the joint lubricated and mitigates the effects of prolonged use. Many of the joint types listed below are also synovial joints.
GLIDING JOINTS are joints like the wrist and ankle where flat surfaces connect and allow for movement in any direction along a plane; the wrist and ankle also have hinge components as described below. The clavicle is a good example of a bone that has only gliding joints.
HINGE JOINTS, like the knee and elbow, allow for a lower range of motion and are limited to a single direction or "plane" of movement, but are stronger and provide more resistance to physical forces/damage.
BALL AND SOCKET joints like the shoulder and hip have the greatest range of motion but are at a higher risk of dislocation or injury owing to their complex structure.
Joint Movement/Position
Joint Movement/Position is described in terms of
- FLEXION is a decrease in the angle between two articulating body parts. e.g. (During flexion, the forearm gets closer to the upper arm.)
- EXTENSION is the opposite: an increase in the angle between two connecting parts. e.g. (Extension is the straightening of the arm.)
- ROTATION is the final movement and is harder to judge; for the shoulder and hips rotations is either medial (towards the midline) or lateral (away from the midline.)
Sprains
A SPRAIN occurs when ligaments, the connective tissues that stabilize and connect joints, are stretched or torn. The most common location for a sprain is the ankle.
Pain, swelling, and bruising are common in sprains. The inability to bear weight or significant point tenderness are warning signs that should prompt an X-Ray evaluation of the injured area. While sprains are rarely emergencies requiring transport, proper care with M.E.A.T (Movement, Exercise, Analgesic, Treatment) can speed recovery. While R.I.C.E. (Rest, Ice, Compression, Elevation) did help alleviate pain it has been shown to decrease and prolong the healing process, however, ice is still recommended immediately after the injury. Since you do not have the ability to X-Ray on the scene, treat the injury by splinting, applying ice, and analgesics as needed and as protocols allow.
Identify a sprain by asking about a sudden "twisting" or painful movement of any joint; a "snapping" or "popping" sensation can also be felt in severe sprains.
Strains
A Strain is the muscular version of a sprain: while sprains affect ligaments, a strain affects the muscles and tendons.
Strains can be muscle pulls, tears, or rupture of the muscle itself. As with sprains, M.E.AT. is an ideal treatment strategy; tendon injuries commonly present with the "snapping" or "popping" sensation described above. As with sprains, strains are rarely emergencies requiring transport; however, severe strains require subacute surgical intervention to avoid permanent disability. If transport is required, treat the injury by splinting, applying ice, and analgesics as needed and as protocols allow.
Fractures


The most common fractures occur in the extremities and collarbone. In general, a bone fracture is not usually a life-threatening injury, but any fracture can be dangerous if it is able to do damage to the vessels and organs around it. So, while a toe fracture is not likely to become emergent, pelvic and femur fractures have a high risk of resulting in serious blood loss.
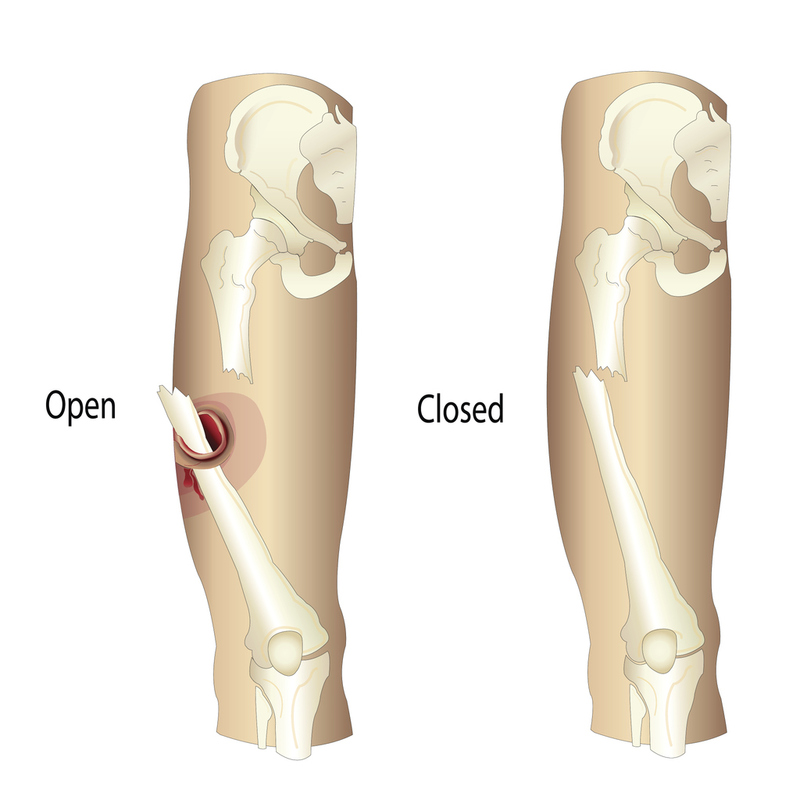
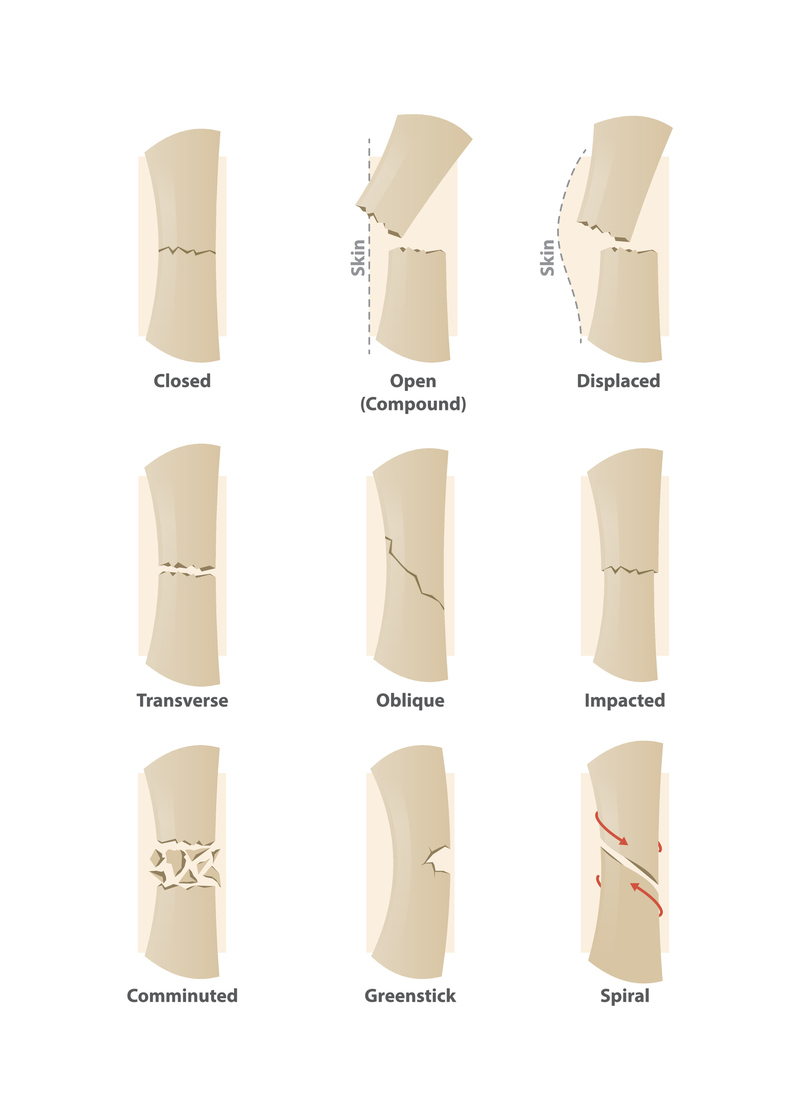
- OPEN FRACTURE: any bone fracture that results in the bone piercing through the skin or being exposed to the environment outside the body. (The term, "compound fracture," is an open fracture, although "open fracture" is preferred due to the other term making it sound like fractures in multiple locations.)
- CLOSED FRACTURE: a bone fracture that does not result in the broken bone breaching the protection of the skin.
As with any trauma that breaks or damages the skin, cover any open wounds with a sterile dressing. This is of particular concern in fractures given the high risk of osteomyelitis, or "bone infection," in patients with open fractures.
Fractures create sharp edges and mobile pieces of bone, both large and small, inside the body; these pieces or shards can sever nerves and vessels or injure tissues around the bone. This secondary mechanism of injury can occur long after the initial trauma.
- TISSUE INVOLVEMENT: The two categories of tissue involvement are "open" or "closed." A closed fracture does not penetrate the skin and can often be managed without surgery, an open fracture invariably requires surgical fixation. Note that open fractures are called "compound" fractures in some cases. This is because there is an obvious bony AND soft tissue injury.
- FRACTURE POINTS: Fractures are either simple or comminuted.
- A SIMPLE FRACTURE has one breakpoint or fracture line.
- A COMMINUTED FRACTURE has multiple fracture lines or bone fragments. Comminuted fractures have a higher risk of damaging surrounding structures such as nerves, blood vessels, and muscles.
- BREAK PATTERN is the most complex category, classified according to the
 break pattern:
break pattern:- GREENSTICK fractures are incomplete fractures only on one side of the bone, caused by an excessive force exerted perpendicularly to the long axis of the bone. Greenstick fractures are mostly found in children due to the increased pliability of their developing bones.
- TRANSVERSE fractures are complete fractures directly perpendicular to the long axis of the bone.
- OBLIQUE fractures are diagonal fractures created when the force applied to a long bone comes from an angle that is not perpendicular.
- SPIRAL fractures occur due to the forced twisting of a bone.
CREPITUS: the sound of bony fragments, separate pieces of bone or disarticulated portions of a joint abnormally rubbing together. (Do not confuse this with subcutaneous crepitus (crepitation), which is air getting into the subcutaneous layers from trauma.)
Management of serious orthopedic injuries
In the field, fractures, dislocations, and severe sprains/strains require stabilization and assessment in the field to minimize further injury.
Fractures and dislocations can lead to nerve damage or limb ischemia due to the stretching/tearing of structures in the injured area.
- Using the "5 Ps" to assess all areas distal to an orthopedic injury both before and after stabilization of an injured area is standard practice.

Pain - Is the amount of pain increasing/decreasing since the time of injury?
Pallor - Is the distal tissue pale or mottled?
Paresthesia - Is there numbness or tingling?
Pulses - Are pulses present?
Paralysis - Does the patient have the ability to move areas distal to the injury?
Clavicular Fractures
Rare complications of clavicular fractures include damage to the subclavian vessels, non-union (faulty healing), and post-traumatic arthritis.
Pelvic Girdle Fractures
Fractures to the complex bones of the pelvis are common in falls and motor vehicle accidents. These injuries can rapidly become fatal due to the large blood vessels running through this area. Vigilance is required to detect these injuries before signs of shock emerge.
- You should be proactive in asking whether the patient has any pain in the pelvic or sacral areas.
- Immobilization of the patient with an external compression splint, pneumatic anti-shock garment, or a diaper splint will provide stability for the injury, reducing the chance of secondary injury.
- When possible, use a scoop stretcher to transfer patients from the floor to the spinal board/vacuum mattress to avoid excessive force on the injured pelvis.
Dislocations
Dislocations occur when the bones themselves are not broken but become dislodged from their proper position at a joint. Dislocations can be hard to distinguish from fractures, as they may both be extremely painful, swollen, and disabling. In a dislocation, deformity or angulation at the location of a joint is often apparent. The bones, while dislocated, can rub together and cause grating or limitation of motion. Other signs and symptoms of dislocation include distal pulselessness, paresthesia, or paralysis due to neurovascular compression at the site of the dislocation.
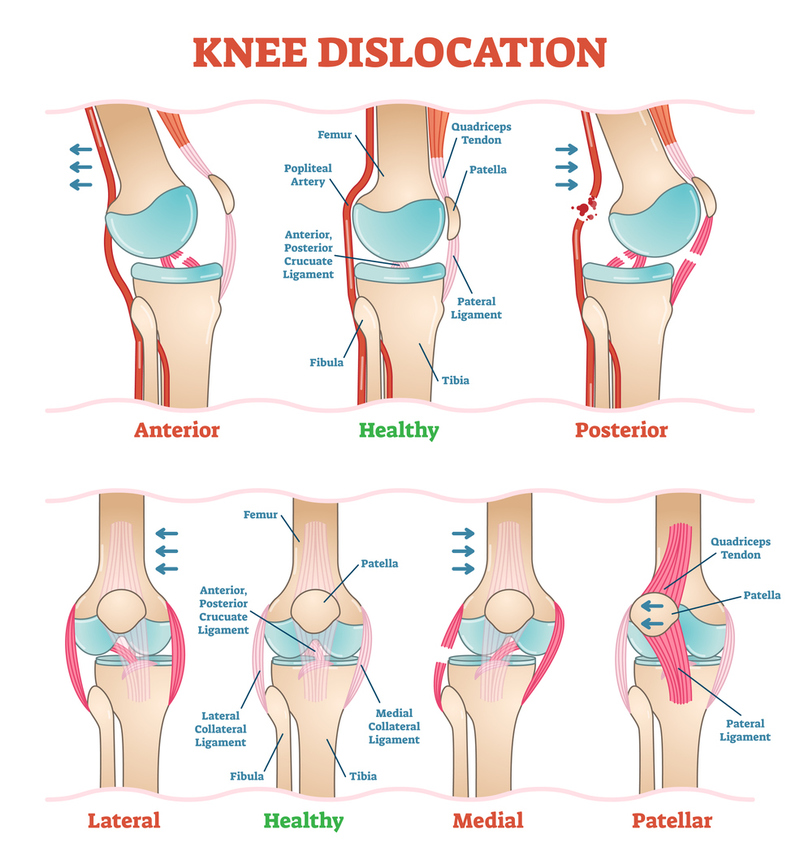
The most common sites for dislocation are the acromioclavicular joint which connects the collarbone to the shoulder, the shoulder itself, the elbow, wrists, and fingers. The hip and knee can also become dislocated. Hip fractures may also cause the hip joint to be unstable and cause the femur to slip out of the socket.
Distinguishing between dislocations and fractures can be difficult. The telltale sign of dislocation would be an obvious deformity, but both share pain, swelling, bruising, and pain. Dislocations can have the effect of locking the joint since the disarticulated portion of the joint is no longer seated in its socket.
There are joints at many locations in the human body which are not entirely obvious. Some of the oft-forgotten are those of the anterior shoulder, namely the acromioclavicular and sternoclavicular joints.
MANAGEMENT:
- Extremity stabilization may be required to prevent movement just as in fracture.
- Make sure to stabilize the injury ABOVE and BELOW the injury site, putting as little pressure as possible on the affected area.
- Cover any open wounds with sterile dressings.
- Once life threats and immobilization measures have been addressed, apply a cold pack, if available, to the deformed area to reduce swelling and pain. Ultimately, pain management is needed by an advanced provider, with definitive treatment being provided at the hospital.
Amputations
An amputation is when a limb or part of a limb has been cut from the body. As a general rule, the more proximal the amputation, the greater the threat to life and the greater the level of care required.
For example, with amputations of a finger, bleeding is much easier to control than when an entire leg is amputated.
MANAGEMENT:
- Elevate the injury
- Apply ice to help slow blood flow.
- Cover the location of the missing body part with a dry, sterile dressing.
- Apply direct pressure (Plan A for hemostasis.)
- Once bleeding is controlled, immobilize the area to prevent further damage to microscopic structures and the disruption of fragile clots.
- If you cannot control bleeding in the stump with direct pressure alone, the use of a tourniquet may become necessary. (Plan B for hemostasis.)

Place these devices as close to the injury as possible while avoiding joints. 1" wide straps are sufficient for the upper limbs 1.5" is the minimum for the lower limbs. Write the time of application on the strap when placing it.
- If you have access to the severed body part, place it in a sealed plastic bag and put that bag in a bowl of ice water and send it to the hospital with the patient.
- Do not put the amputated body part directly onto the ice and do not let the amputated part become saturated with water. All amputated body parts should be saved even if they appear unsalvageable as the part may become valuable material for plastic surgeons to reconstruct other damaged parts of the patient's body.