Test Complete
- Questions
- Score
- Minutes
| Overall Results | |
|---|---|
| Total Questions |
| Category Results | |
|---|---|
Compartment Syndrome
Category: Trauma
Topic: Orthopedic Trauma
Level: AEMT
Next Unit: Achilles, Patellar, and other Tendon Injuries
17 minute read
Pathophysiology
Compartment syndrome is a condition that results from increased pressure within the fascial layers that the muscles are grouped into--the "compartments" after which the syndrome is named.
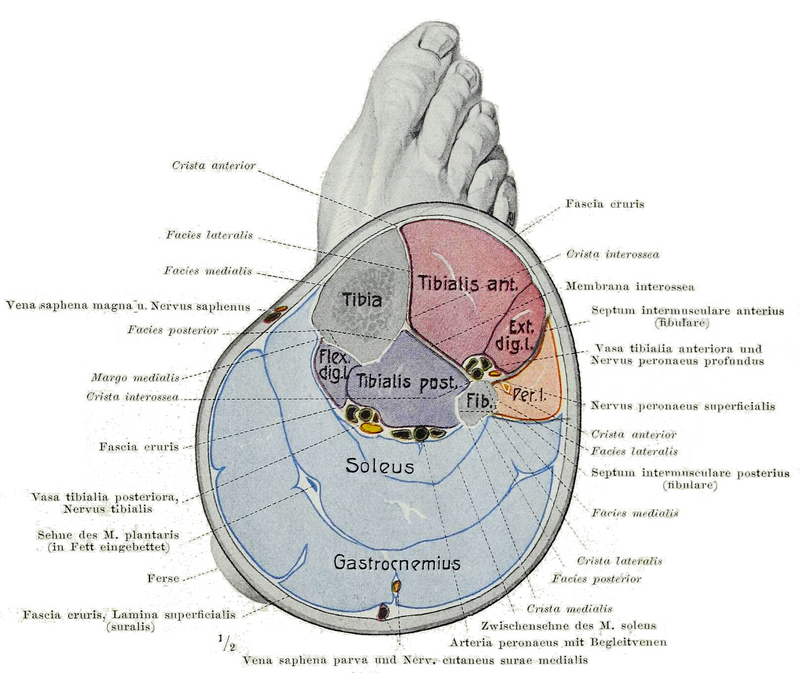
Generally, a compartment consists of the muscles that perform a specific action and their associated nerves/vessels. For example, the posterior compartment of the lower leg contains the muscles that flex the knee and extend the foot, along with the major blood/nerve supply of the foot.
In order to understand how this syndrome occurs, we will explore
- common injuries,
- the effects of increased pressure, and
- some special situations
INJURIES: Fractures and their casting are the most common cause of compartment syndrome.
- Tibial, humeral, and radial/ulnar fractures account for the majority of compartment syndromes due to the small space and complex vascularity of these areas.
- The more proximal limbs are commonly involved in the setting of significant crush injuries, which can cause muscle damage and enough swelling to overcome the larger sizes of these compartments.
- Finally, significant burns are another common cause of compartment syndrome.
Any soft tissue injury mediated by toxins, overexertion, medication, and even immobilization can result in compartment syndrome.
PRESSURE: The root problem in compartment syndrome is a lack of perfusion to the tissues and resultant ischemia leading to the death of muscle/nerves. The capillaries push blood forward at a pressure of 20 mmHg, with the normal compartment pressure usually being < 10 mmHg. This gradient, once breached, will stop blood flow.
Irreversible injury begins 4 hours after the onset of ischemia, resulting in muscle breakdown and neuron degeneration.
SPECIAL SITUATIONS: Snakebites, casts, and muscle breakdown complicate compartment syndrome.
- Snakebites commonly occur on the forearm and lower leg, and these areas are already predisposed to compartment syndrome when injured. Venom from some species of snakes has a high likelihood of causing dramatic and rapid tissue swelling. If possible a picture or the body of the animal should be brought for identification and administration of appropriate antivenin.
NOTE: Sucking on the wound, applying tourniquets, and pouring substances onto the wound is not effective.
- CASTS, just like snakebites, are most commonly placed on the forearm and lower leg--hotspots for compartment syndrome. These are often placed shortly after fracture, which can cause compartment syndrome. Casts (and splints!) act to lower the amount of swelling, raising the compartment pressure above the ischemic threshold. This can occur at any time after a cast has been placed! However, it is most common in the first 12 hours of cast wear.
- MUSCLE BREAKDOWN (Rhabdomyolysis): a state where the membranes surrounding the muscle fibers become unstable and spill a nephrotoxic (kidney-killing) protein into the blood. It often goes hand-in-hand with crush injuries and compartment syndrome.
- The longer and more severe the ischemia, the more rhabdo occurs;
- The sicker and more dehydrated the patient, the more deadly rhabdo is to the kidneys.
- Isotonic bicarbonate can be used to prevent (and treat) acidosis due to biochemical alterations from the toxins and counteract hyperkalemia.
Minutia you don't need to know:
Pathology of "crush syndrome": crushed muscle releases intracellular calcium → mitochondrial dysfunction → ATP production dysfunction → lactic acid buildup and sodium/potassium and calcium pump dysfunction (necessary for myocyte integrity) → myocyte death → release of intracellular muscle creatine kinase (CK), muscle enzymes, myoglobin, and various electrolytes, which cause acute tubular necrosis of the kidney.
What you need to know:
Compartment syndrome and crush syndrome cause rhabdomyolysis (muscle cell death) which releases myoglobin into the circulation which is toxic to the tubules of the kidney → acute kidney injury → acute kidney failure.
Assessments
Following an initial survey of the scene and the ABCs, compartment syndrome is recognized by a thorough inspection or any and all areas of injury. Your suspicion should be raised if the patient has one of the injuries listed above, has a known disorder that predisposes them to bleeding, or has a fracture in the high-risk areas listed above.
Pain is your key symptom: you cannot have compartment syndrome without pain.
This pain will NOT be relieved by keeping the injured area still and can be dramatically more than the initial pain from the injury!
THE 5 Ps: The 5 Ps are your guide to the severity and recognition of compartment syndrome.
The more P's present, the more likely this is compartment syndrome. (However, only pain is required to suspect developing compartment syndrome!)
- Pain: dramatically worse with passive stretching!
- Pallor: lack of blood flow turns the area ghostly pale.
- Pulseless: as above.
- Paralysis: nerve compression prevents signal transmission.
- Paresthesia: as above.
The timeline of compartment syndrome is as follows
- Swelling of the tissues makes the area appear firm ⇒
- Pain develops in increasing severity as compared to the initial injury (due to the stretching of sensitive nerves) ⇒
- Pulses disappear as pressure exceeds even that of the large blood vessels ⇒
- Sensation disappears and paresthesias "tingling" begin, as nerves lose the ability to conduct ⇒
- Total paralysis occurs as severe pain prevents movement and muscles lose the ability to contract.
Management
Managing compartment syndrome in the field revolves around supporting, minimizing, and transporting.
SUPPORTING: Provide pain control as your protocols and level of training permit:
- Elevate to the level of the heart with the elbow extended, supported by a pillow
- Maximize IV hydration to the safest amount possible; this is one of the only ways to prevent kidney damage from significant rhabdomyolysis and systemic complications from acidosis, which is secondary to lactate production by ischemic tissue. Remember to consider sodium bicarb [SEE ABOVE].
- Back off of IV hydration if shortness of breath or edema of uninjured limbs develops.
MINIMIZING:
- Remove any casts/splints/compression in the area.
- Ensure that the limb is at the level of the heart to minimize swelling.
- If the forearm is involved, ensure the arm is straight!
- Manage any other co-dominant injuries to minimize the chance of complications.
TRANSPORTING: Definitive treatment of compartment syndrome requires measurements of pressure within the limb via specialized tools and rapid surgery to open each compartment to allow the swelling to abate naturally. This process is especially gory and may horrify patients, but otherwise healthy patients tend to heal and recover well with time.
- Transport time is one of the most important prognostic factors in these patients.
- If you suspect compartment syndrome, notify dispatch or the trauma team present in the ED--the minutes you save matter!