Test Complete
- Questions
- Score
- Minutes
| Overall Results | |
|---|---|
| Total Questions |
| Category Results | |
|---|---|
Cardiac Anatomy and Function
Category: Cardiology
Topic: Cardiovascular Anatomy and Physiology
Level: Paramedic
Next Unit: Regulating Blood Flow
25 minute read
Layers of the Heart
The heart wall has three layers, going from innermost to outermost:
- Endocardium
- Myocardium
- Pericardium
ENDOCARDIUM
The endocardium is the inner lining. (Endo- means "lining.") It is the layer of cells that are exposed to the blood within the 4 chambers and which lines the heart valves.
MYOCARDIUM
The myocardium is the middle and thickest layer of the heart wall. (Myo- means "muscle.") Most of the heart wall is the myocardium. It also houses the cardiac electroconductive system (SA node, AV node, HIS fibers, and Purkinje fibers).
PERICARDIUM: makes up the outer layers of the heart wall, enclosing the heart. (Peri- means "around" or "surrounding.")
- The inner portion of the pericardium is a two-layered sac called the serous pericardium. The VISCERAL PERICARDIUM (or epicardium) is closely adherent to the underlying myocardium and is reflected upon itself (doubles back on itself) to form
- the outer PARIETAL PERICARDIUM, which lines a fibrous sac*. Between the two layers of the serous pericardium lies the PERICARDIAL CAVITY which normally contains up to 50 mL of pericardial fluid.
*It also has a tough fibrous layer, called the Fibrous Pericardium, external and adherent to the parietal pericardium
Going from innermost → outermost, therefore:
Endocardium → Myocardium → Visceral pericardium ("epicardium") → Pericardial Fluid → Parietal Pericardium → Fibrous Pericardium
Diseases Involving the Heart Wall
Systemic Inflammatory Disease can affect the endocardium (valvular disease, thrombi), the myocardium (myocarditis, cardiomyopathy, rhythm and conduction disturbances, heart failure), coronary arteries (acute coronary syndromes, ischemic heart disease), and the pericardium (pericarditis and pericardial effusion).
ENDOCARDIUM: Besides inflammatory disorders, the endocardium can also be affected by:
- Endocarditis: Normally resistant to organisms (infection), if the endocardium is injured, an initially sterile platelet-fibrin complex can become infected. The bacterial source for endocarditis may be a dental abscess, infected skin lesion, infected vascular catheter, or from minor trauma of the oropharyngeal, gastrointestinal, or genitourinary mucosa.
- Bundle Branch Block: The right bundle branch is vulnerable to stretch and trauma for two-thirds of its course when it is near the subendocardial surface.
MYOCARDIUM: Besides inflammatory disorders, the myometrium can also be affected by:
- Myocardial Ischemia and Infarction (MI), causing heart muscle death.
- "Stunned" myocardium is characterized as transient post-ischemic dysfunction, after an episode of acute ischemia.
- "Hibernating" myocardium is characterized as chronic, but potentially reversible, ischemic dysfunction.
- Subendocardial infarct: Subendocardial infarctions affect only the inner layer of the myocardium and typically present as non-ST elevated myocardial infarctions (NSTEMIs) without pathological Q waves.
- Congestive Heart Failure: muscle weakness leading to ineffective pumping function.
PERICARDIUM: Besides inflammatory disorders, the pericardium can also be affected by:
- Cardiac Tamponade is when there is an abnormal accumulation of pericardial fluid under pressure, impairing cardiac filling and creating hemodynamic compromise. It can be caused by malignancy, myocardial infarction, infection, and collagen vascular disease.
Blood Supply to the Heart
Like any organ, the heart's cells require oxygen, and like the other tissues of the body, this oxygen is supplied via a blood supply. The heart has a specialized vascular system to supply blood to the muscle ("myocardial) cells that make up the myocardium (heart muscle) itself, called the coronary circulation, and to the conduction system. The coronary arteries originate as the right and left main coronary arteries which exit the ascending aorta just above the aortic valve (as coronary ostia).
It is comprised of two major coronary arteries: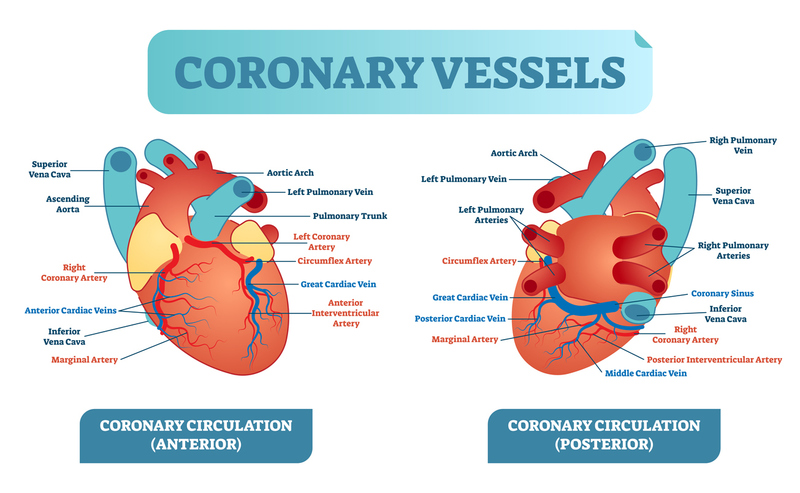
- Left coronary artery (LCA): each of its 2 branches supplies blood to the left atrium and parts of the left ventricle.
The LCA branches off into --Left anterior descending (LAD) artery; and the Circumflex artery (Cx).
- Right coronary artery (RCA): supplies blood to the right atrium, right ventricle, the bottom of the left ventricle, and back of the intraventricular septum. Its branches are:
Posterior descending artery (PDA); and the Marginal artery.
There are also anastomoses in the heart that create a normally dormant collateral circulation which can open when the coronary vessels become occluded.
The LAD distributes blood to the conduction system within the heart as well as to the left and right ventricles. Therefore, an MI from LAD blockage often presents as heart block.
Venous System: The coronary circulation also includes the coronary sinus and great cardiac vein, through which deoxygenated blood is sent back through the circulation system to be reoxygenated.
Overview of Stroke Volume, Cardiac Output, and Starling's Law
STROKE VOLUME: the volume of blood pumped from the left ventricle over the aortic arch with each contraction, as a function of 3 components:
- Preload: The end-diastolic volume.
- Myocardial Contractility: The strength of contraction during systole.
- Afterload: The pressure against which the heart must work to eject blood during systole.
The normal stroke volume is typically around 70 ml for a healthy adult.
CARDIAC OUTPUT: a measurement that analyzes the effectiveness of the heart--specifically the amount of blood put out by the left ventricle in one minute--and is calculated as heart rate multiplied by stroke volume--
(HR x SV = CO).
STARLING'S LAW OF THE HEART: states that the stroke volume of the heart increases in response to an increase in the volume of blood filling the heart (the end-diastolic volume) when all other factors remain constant.
Starling’s Law is effective when attempting resuscitation, administering fluids in an effort to increase stroke volume, which then results in increased cardiac output.
Preload vs Afterload
Preload vs afterload is a common source of confusion.
(Systemic Vascular Resistance) SVR → Afterload → Preload (end-diastolic volume) → Inotropy → Stroke Volume
PRELOAD is a VOLUME (end-diastolic volume). It is the volume of blood in the ventricle after being filled during ventricular diastole, which--and do not get confused--occurs via the atrium ejecting blood through the mitral valve during the atrial systole.
AFTERLOAD is a PRESSURE. Once the left atrium has sent its load of blood through the mitral valve into the left ventricle, the pressure within the ventricle becomes high enough to push back against the flaps of the mitral valve, closing it; ideally, with contraction (inotropic), the pressure will be enough to blow open the aortic valve to allow a volume of blood to leave the ventricle in one stroke (one contraction) or, the "stroke volume."
Afterload (remember, "pressure") is determined by the Systemic Vascular Resistance (SVR). (In the right ventricle, afterload is determined by pulmonic vascular resistance.) Therefore, SVR, against which the ventricular blood must overcome to leave the ventricle, is the pressure exerted against the aortic valve by the rest of the body's vascular pressure against it. In this question, vasoconstriction, kindly offered in the prompt as an "increase the systemic blood pressure during hypovolemia," increases the resistance against which the left ventricle must oppose to blow open the aortic valve and send blood onward from the heart.
Vasoconstriction, by reducing the cross-sectional area through which the blood flows, increases the amount that remains in the heart after the contraction (the afterload). This, in turn, increases the preload volume, from the next contraction's point of view, which increases the inotropy, pumping up the stroke volume. (Stretched myocardial fibers stimulate stronger contractions.)
The DIRECT result of vasoconstriction, (that is, increasing the systemic pressure to be overcome) is increased afterload--that is, the increased systemic pressure which the ventricle must overcome to continue pumping.
This pressure--the afterload--is contained in the volume--the preload-- as related to the next contraction; volume distends, and the ventricle--thanks to the preload--will beat stronger due to the increased stretch on the myocardium from the secondary increased preload (from the primarily increased afterload).
SVR → Afterload → Preload (end-diastolic volume) → Inotropy → Stroke Volume
Preload is largely determined by cardiac return, and increasing the pooling of blood in the veins will dramatically lower cardiac return. (This is the physiology behind orthostatic hypotension, in which a sizeable proportion of total blood volume can pool in the legs when standing suddenly.)
Since preload is a volume, pooling of blood on the venous side means less that gets back to the heart, which means a lower preload. (Afterload is pressure and its relation to peripheral vascular resistance--an arterial phenomenon, not a venous one.)
Peripheral venous vasodilation leads to the lethal positive feedback that kills patients who decompensate in the setting of shock:
Venous vasodilation → decreased cardiac return → low preload (and less stretch on myocardial fibers) → lower inotropy (strength of contraction) → lower stroke volume → even lower blood pressure (+ the decreased cardiac return) → lower preload →→→ etc. → death.
SVR → Afterload → Preload (end-diastolic volume) → Inotropy → Stroke Volume:
Technically, preload and afterload, while being apples (volume) and oranges (pressure), are interrelated, as a lower preload → lower inotropy → functionally, a lower afterload (the pressure needed to blow the aortic valve open against the systemic circulation); and a lower afterload will → less cardiac output → less cardiac return (lower preload).
The Exception
Dextrocardia is a rare congenital defect where the heart is situated primarily on the right side of the body instead of the left. (In "situs inversus totalis," all of the organs are reversed, which technically makes dextrocardia in these individuals a normal variation. As might be expected, there are ECG changes due to the normally placed electrodes over the differently positioned heart.
These changes can be reversed by placing the precordial leads in a mirror-image position on the right side of the chest and reversing the left and right arm leads. However, in the field, you won't be dealing with this. Just know what dextrocardia is.
Other cardiac anomalies will be well known by the patient--your EMS call won't be his/her first!