Test Complete
- Questions
- Score
- Minutes
| Overall Results | |
|---|---|
| Total Questions |
| Category Results | |
|---|---|
Anaphylaxis
Category: Medical
Topic: Immunology
Level: AEMT
Next Unit: Epinephrine as a Treatment for Anaphylaxis
23 minute read
Anaphylaxis, Mast Cells, and IgE
The incidence of common or major immune system disorders in the United States, including anaphylaxis, varies by reporting agency but is estimated to be between 50-200 episodes per 100,000 people per year, with upwards of 1,500 deaths per year. Both the incidence and prevalence are increasing.
Children have a five times higher morbidity and hospitalization rate than adults. Other immune system disorders include collagen vascular disease, hypersensitivity, and transplant disorders.
Anaphylaxis vs. Anaphylactoid Reactions
(Immunologic vs. Nonimmunologic Anaphylaxis)
ANAPHYLAXIS IgE- and Mast Cell-Mediated
Anaphylaxis is defined as a serious allergic or hypersensitivity reaction that is rapid in onset and may cause death. It is an acute, life-threatening, systemic syndrome caused by the sudden release of mast cell mediators into the systemic circulation. Even a very limited exposure to a very small amount of allergen can trigger anaphylaxis.
Allergic reactions, in contrast, are localized to one or several areas of the body and are rarely life-threatening.
In anaphylaxis, mast cells (and basophils) and IgE are THE problem.
"ANAPHYLACTOID" REACTIONS Not IgE-Mediated.
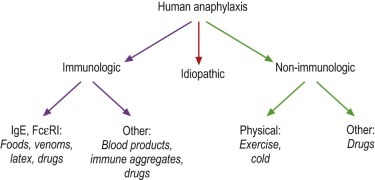
Anaphylactoid reactions are defined as those reactions that produce the same clinical picture as anaphylaxis but
- are not IgE-mediated,
- occur through a direct non-immune (not IgE-provoked) release of mediators from mast cells and/or basophils,
- nor result from direct complement activation.
They result from exercise, exposure to cold, radiological contrast media, etc.
Because anaphylaxis and anaphylactoid reactions can be clinically indistinguishable, the World Health Organization has discarded these two names and now refers to them as:
Immunologic Anaphylaxis ("Anaphylaxis") and Nonimmunologic Anaphylaxis ("Anaphylactoid")
The reason for this change is that many assumed that anaphylactoid reactions were less severe, which is not the case. The WHO, therefore, called both of them "anaphylaxis," with the two sub-types.
Mast Cells
MAST CELLS play a major role in allergic responses (response to allergen challenge), including
- anaphylaxis (discussed here),
- urticaria,
- asthma,
- rhinitis, and
- atopic dermatitis.
Mast cells come from stem cells that reside in the bone marrow and spleen, and they end up in varying numbers in practically all tissues. They are positioned as sentinels at the body's portals of entry within mucosal membranes lining the respiratory, digestive, and urogenital systems, throughout the dermis, and surrounding blood vessels. Mast cells reside within the connective tissue of these and all vascularized organs.
Their highest density is at the interfaces between the internal and external environments where they can respond to foreign organisms and antigens, providing a sentinel function.
Mast cells contain cytoplasmic granules, containing macromolecular complexes of proteoglycans and proteases. As an important part of the innate immune system, they assist in the innate defense against certain bacterial and viral infections by releasing pro-inflammatory cytokines. They also produce antimicrobial peptides which disrupt microbial membranes.
Mast cell-derived cytokines--especially tumor necrosis factor (TNF)--result in early and effective recruitment of neutrophils and other leukocytes to sites of infection.
They also activate complement.
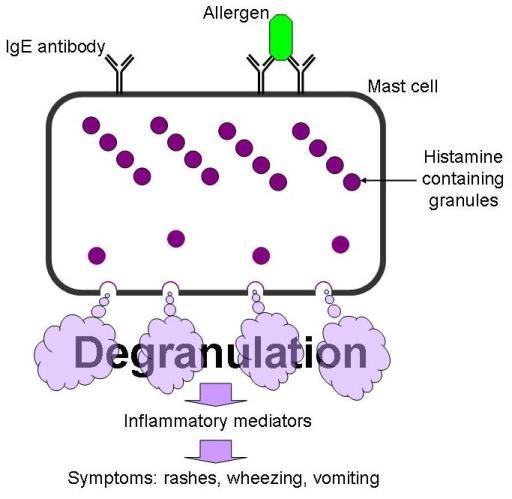
The degranulation of mast cells (and basophils) results in the systemic release of various biochemical mediators and chemotactic substances, including:
- Histamine, serotonin, tryptase, chymase, and heparin, which are substances inside the granules.
- Histamine-releasing factor and other cytokines.
- Newly-generated mediators such as prostaglandin, leukotriene, platelet-activating factor (PAF), and leukotrienes.
Mast cells in allergy: Activation results in both an early and a delayed phase of inflammation.
Mast cells--the downside: besides anaphylaxis, mast cells probably play a role in autoimmune diseases such as rheumatoid arthritis and multiple sclerosis.
IgE
Allergen-specific IgE is integral to the pathogenesis of allergic disorders. Sensitization refers to the production of allergen-specific IgE (although the term allergy isn't correct unless there are signs and symptoms).
How to make IgE:
Once a substance
- enters the body through ingestion, inhalation, or injection, it is
- degraded into allergens, and these
- allergens (usually proteins but occasionally carbohydrates) are taken up by antigen-presenting cells (APCs--macrophages, dendritic cells, B-cells), then
- APCs further degrade the allergen and present peptide fragments of it on the cell surface which are recognized by Th2 T-helper) cells.
- Th2 cells then interact with B-cells and stimulate them to mature into plasma cells that
- produce IgE specific to the component of the allergen in question.
B cell maturation primarily occurs within mucosal lymphoid tissue.
Mast cell activation occurs via the IgE receptor where IgE is linked to an antigen. This is a strong stimulus for degranulation and release of preformed mediators, as well as the production and subsequent release of leukotrienes, prostaglandins, and cytokines, including numerous chemokines.
Anaphylaxis
Anaphylaxis is a sudden and severe allergic reaction that occurs within minutes of exposure. It is a rapidly progressing, life-threatening systemic allergic reaction and most often results from IgE-mediated reactions to foods, drugs, and insect stings, but any agent capable of inciting a sudden, systemic degranulation of mast cells can produce it.
Common causes of anaphylaxis are:
- penicillin,
- peanuts,
- tree nuts,
- wheat,
- fish,
- shellfish,
- milk and eggs, and
- insect stings (bees, yellow jackets, wasps, hornets, fire ants, etc.).
Anaphylaxis is an acute systemic (multi-system) and severe Type I Hypersensitivity allergic reaction.
In a type 1 hypersensitivity, the antibody is IgE instead of IgA, IgG, or IgM.
Hypersensitivity reactions are classified into the following 4 types:
Type I: immediate hypersensitivity reactions that involve immunoglobulin IgE–mediated release of histamine and other mediators from mast cells and basophils. Example: anaphylaxis.
Type II: cytotoxic hypersensitivity reactions that involve IgG or IgM antibodies bound to cell surface antigens, with subsequent complement fixation. Example: drug-induced hemolytic anemia.
Type III: immune-complex reactions involve circulating antigen-antibody immune complexes with subsequent complement fixation. Example: serum sickness (reaction to proteins in antiserum derived from a non-human animal source, occurring 5–10 days after exposure).
Type IV: delayed hypersensitivity reactions, cell-mediated immunity, mediated by T cells rather than by antibodies. Example: contact dermatitis from poison ivy or nickel allergy.
Signs and Symptoms
- severe respiratory distress or wheezing,
- rapid pulse and low blood pressure,
- pale, red, or cyanotic skin,
- hives,
- itching,
- swelling around eyes, mouth or tongue,
- altered mental status, and
- nausea and vomiting.
Complications, besides death, include biphasic anaphylaxis, which can occur in 1 out of 5 cases of anaphylaxis, and shock.
DEFINITION, BIPHASIC ANAPHYLAXIS: recurrence of symptoms that develop after resolution of the initial anaphylaxis without additional exposure to the trigger
and
Shock: both distributive and hypovolemic shock (with tachycardia): organ system failure due to shock-heart, shock-vasculature, shock-lungs, resulting in circulatory collapse or respiratory arrest.
Management
Immediate medical attention is needed for this condition. The primary cause of mortality in anaphylaxis is airway compromise and/or cardiovascular collapse. It can get worse very, very fast and lead to death within 15 minutes if treatment is not received.
To emphasize this, in fatal anaphylaxis, median times to cardiorespiratory arrest are
- 5 minutes in iatrogenic anaphylaxis,
- 15 minutes in stinging insect venom-induced anaphylaxis, and
- 30 minutes in food-induced anaphylaxis.
EMR Management of a patient in anaphylaxis includes
- airway maintenance,
- oxygen administration,
- proper positioning,
- monitoring of vital signs,
- removal of allergen (if possible), and
- determining whether or not the patient has used his/her epinephrine auto-injector.
EPINEPHRINE IS THE FIRST AND MOST IMPORTANT TREATMENT FOR ANAPHYLAXIS, administered as soon as anaphylaxis is recognized to prevent progression.
Delayed epinephrine injection is associated with fatalities.
In the Field
In the field, the following are important steps:
- Remove the inciting antigen if possible.
- Epinephrine, IM, IV, or via autoinjector.
- Any patient whose hypotension does not respond to epinephrine should receive large volume fluid resuscitation (normal saline).
- Bronchodilators treat bronchospasm unresponsive to epinephrine but are only adjunctive therapy because alone they won't prevent edema in the upper airway or shock, for which the alpha-1-adrenergic effect of epinephrine is needed.
- 2 large-bore IV for both medication and volume resuscitation.
- Adults should receive 1-2 liters of normal saline at the most rapid flow rate possible in the first minutes of treatment. Large volumes of fluid (e.g, up to 7 liters) may be required.
- Children should receive normal saline in boluses of 20 mL/kg, each over 5 to 10 minutes, and repeated, as needed.
- Supine position with legs elevated. An upright position should be used only if the supine position combines with airway swelling to prevent ventilation.
Lips, tongue, and oral pharynx are assessed for angioedema, and the patient is asked to speak his or her name to assess peri-glottic or glottic swelling.
If the upper airway is not edematous, the patient should be placed in the recumbent position with the lower extremities elevated to maximize perfusion of vital organs (pregnant patients on their left side).
- O2 (nonrebreather mask, 15 L/minute--70-100%)
Intubation if the airway is compromised.