Test Complete
- Questions
- Score
- Minutes
| Overall Results | |
|---|---|
| Total Questions |
| Category Results | |
|---|---|
Alzheimer Disease
Category: Special Populations
Topic: Geriatrics
Level: EMT
Next Unit: Dementia, Delirium, and Confused States
16 minute read
Definitions & Epidemiology
ALZHEIMER DISEASE (AD): is a neurodegenerative disorder of uncertain cause and pathogenesis that primarily affects older adults and is the most common cause of dementia.
Approximately 5.5 million people in the US are affected by Alzheimer’s and it has the earliest onset of senility of all senile diseases.
DEMENTIA, based on the criteria:
Significant acquired cognitive impairment that interferes with independence and affects at least one of the following:
- Learning and memory
- Language
- Executive function
- Complex attention
- Perceptual-motor function
- Social cognition
► Alzheimer's disease (AD) is the most common form of dementia in older adults, accounting for 60-80% of cases.
Dementia in AD has an insidious onset and is progressive. Treatments are available that ameliorate some symptoms, but there is no cure or disease-modifying therapy (treatment that slows the course of the illness) currently available, and the disease inevitably progresses. There are no survivors.
The prevalence of AD doubles every 5 years over the age of 65.
Early-onset AD (onset of symptoms < 65 years of age) is unusual, and many of these patients present for evaluation due to concerns about job performance.
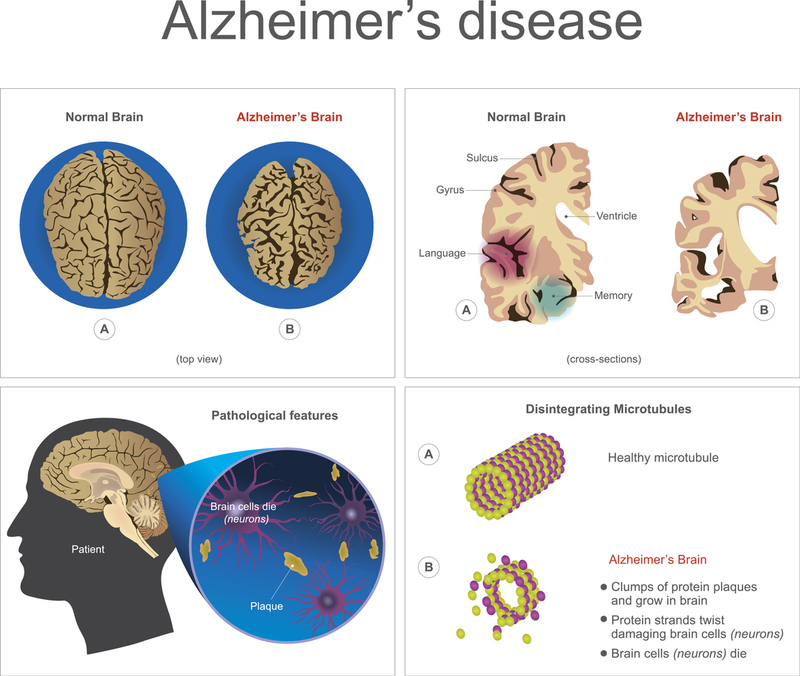
CAUSE: the exact mechanisms remain unclear and are the subject of on-going research, but all forms of AD seem to involve excessive amounts of amyloid beta peptides in the brain--from overproduction and/or decreased clearance. Abnormal clusters of these chemically “sticky” proteins are called "plaques," which can clump together as tangles that are prime suspects in cell death and tissue loss.
Stages
AMNESIC MILD COGNITIVE IMPAIRMENT (MCI): a state of long-term memory impairment of new information, while general cognitive and social functioning are preserved. MCI is considered an early stage of AD, with conversion to AD dementia at 10-15%/year.
PRECLINICAL STAGES: based on the Clinical Dementia Rating Scale:
- Stage 1--asymptomatic amyloidosis.
- Stage 2--amyloidosis + neurodegeneration, with cortical thinning and hippocampal atrophy.
(The hippocampus is important to memory.)
- Stage 3--amyloidosis + neurodegeneration + subtle cognitive decline.
CLINICAL STAGES:
- MCI--amnestic mild cognitive impairment.
- Alzheimer Disease Dementia.
Diagnosis
AD dementia is diagnosed based on a criteria list that meets the definition of dementia, excludes delirium, psychiatric disorders, but demonstrates impairment of at least 2 of the following:
- impaired ability to acquire and remember new information;
- poor judgment, especially in handling complex tasks;
- impaired visuospatial ability;
- impaired language;
- personality or behavior changes.
Prognosis
AD is fatal.
Life expectancy after a diagnosis of AD ranges from 3-11 years, depending on how impaired the person is at the time of diagnosis. Patients generally die from terminal-stage complications of advanced debilitation, such as dehydration, malnutrition, and infection.
Signs and Symptoms
Most commonly, memory impairment is first, followed by executive dysfunction and visuospatial impairment. Language and behavioral changes come later.
MEMORY
Declarative episodic memory (memory of events occurring at a particular time and place) is usually profoundly affected in AD.
Memory for facts such as vocabulary and concepts (semantic memory) often becomes impaired somewhat later.
Memory for recent events is prominently impaired in early AD.
BEHAVIOR
Psychiatric symptoms are common in the middle and late course of the disease. Beginning with subtle symptoms such as apathy, social disengagement, and irritability, but can progress to agitation, aggression, wandering, and psychosis.
Caveat: Apathy can be difficult to distinguish from depression, which should be identified because depression is treatable.
Apraxia (difficulty performing motor tasks) and sleep disturbances can occur.
Normal day-to-day living with AD may include problems associated with management, patient violence, patient verbal abuse, and fearful patients.
COMPLICATIONS
Seizures in 10-20% of cases, primarily focal nonmotor with impaired awareness. Examples: Accidents, wandering, abuse from others.
MEDICATIONS
Alzheimer’s treatment includes cholinesterase inhibitors, NMDA-antagonists, antipsychotics, and antidepressants.
Early AD is treated with cholinesterase inhibitors. More advanced disease is treated with NMDA-antagonists, such as Memantine.
AD patients have decreased neurotransmitter acetylcholine, and cholinesterase inhibitors inhibit its breakdown.
Cholinesterase inhibitors, besides causing bradycardia and hypotension, can cause sleep disturbances that get confused with AD behavioral changes.
NMDA-antagonists have side effects that can be the same as the cognitive changes in AD patients, misleading one to think the AD S&S are getting worse when in reality it is just a side effect that is being observed.
Management
In the field, management of AD may include communication, slow clear instructions, distraction and redirection from agitation, and other strategies. Treat the patient symptomatically and consider co-illnesses as well as medication reactions.
Because AD patients can exhibit behavior ranging from apathy to irritability to combativeness, they are not only difficult to deal with, but their behavior may have provoked retaliation from caregivers and family, presenting as a different emergency altogether--trauma. Additionally, their impaired awareness and tendency to wander may create tragic accident scenarios.
You may also be called to see them for complications of poor hygiene or living conditions when they live alone or with someone incapable of caring for them properly.
SAFETY FIRST: In the course of your responding to a call, you may be exposed to verbal abuse and possibly even patient violence, so your first responsibility is scene safety.
The patient's mental changes may include fear and confusion, which requires:
- Reassurance
- Slow clear instructions
- Distraction techniques to mitigate agitation
Caveat: many conditions can mimic AD in the elderly, including hypoglycemia, medication errors, co-illnesses, AD treatment itself (prescribed cholinesterase inhibitors and NMDA-antagonists), antipsychotics, antidepressants, or medication interactions.
Treatment
As an EMS responder, your first obligation is scene safety (as in any situation involving cognition impairment).
Your next obligation is to treat acute symptoms if indicated. Fall trauma, abuse, accidents, etc., are all part of the AD picture and will be what you are primarily called for, as most patients will have a history of dementia as a chronic condition you cannot impact.
However, if there is no prior history and you are called for a sudden change from normal behavior to behavior some might associate with AD, it warrants rapid transport to rule out non-AD causes, such as stroke, medication interactions, or new medical issues, with support en route for ABC (airway, breathing, circulation), reassurance, and IV access.