Test Complete
- Questions
- Score
- Minutes
| Overall Results | |
|---|---|
| Total Questions |
| Category Results | |
|---|---|
Advanced Spinal Cord Injuries
Category: Trauma
Topic: Nervous System Trauma
Level: Paramedic
Next Unit: Intracranial Hemorrhage
20 minute read
Pathophysiology
The pathophysiology of spinal cord injury is based around the disruption of axons or cell bodies within the cord. There are many mechanisms that can result in acute injury: they are grouped into mechanical, vascular, and infectious causes.
The most common etiology is trauma: excess flexion, compression, rotation, lateral bending, and direct laceration are common mechanisms of injury.
More specific causes are
- Distraction: Transverse fracture or dislocation, commonly due to a seat belt lap band that is too high.
- Concussion: A massive trauma that somehow spares the spinal vertebra can still cause concussion and contusion of the cord contained within.
- Compression: A slipped disk or fractured vertebra can squeeze on the cord and prevent effective signal transmission.
Cord lesions generally present as complete or partial deficits.
-
COMPLETE DEFICITS result in total loss of sensation and voluntary motor function below the level of the lesion.
Total cord lesions tend to be complicated by significant hypotension (neurogenic shock), paralytic ileus, and autonomic dysfunction; this is due to the imbalance between the parasympathetic and sympathetic nervous systems as a result of the transaction. -
The PARTIAL CORD SYNDROMES present with variable deficits based on the positions of the neurons in the spinal cord; they are as follows:
- Brown-Sequard’s syndrome is due to laceration of one half of the spinal cord. It results in paralysis and loss of positional sense on the side of the injury with loss of pain and temperature sensation on the opposite side.
Pain and temperature sensation enters the spine but crosses over to the other side before ascending to the brain, whereas positional sense and motor are innervated on the same side.
- Anterior cord syndrome causes loss of voluntary motor function and pain/temperature sensation below the lesion, basic touch and proprioception are left intact. This can occur due to damage to the cord itself or the artery that runs along its ventral aspect.
- Central cord syndrome is the most common partial deficit, hyperextension injuries and hyperflexion injuries (whiplash) are common causes. It results in weakness that is far greater in the upper limbs as opposed to the lower ones. With central cord syndrome, there is a highly variable sensory loss.
Spinal Shock
In spinal shock conduction in the cord is impeded by swelling and neuronal damage due to loss of potassium in the cord cells into the extracellular fluid, which reduces nerve transmission.
- It begins at the time of injury and involves the entire cord below the level of injury.
- As the potassium levels balance between the intracellular and extracellular fluids, improvement begins. Spinal shock can last 7 to 20 days.
Spinal shock may result in
- "autonomic hyperreflexia,"
- absent bowel and bladder control,
- bradycardia, and
- hypotension.
A transient paralysis may also occur with the total loss of all reflexes and voluntary movement below the lesion. Spinal shock does not imply permanent paralysis has occurred.
AUTONOMIC DYSREFLEXIA (Above T6)
20-70% of those with spinal cord injury above T6 develop autonomic dysreflexia (hyperreflexia), which is loss of normal autonomic responses for heart rate and vascular tone. It usually occurs within a month to a year after the injury, but it doesn't happen with injuries lower than T6.
- Sympathetic responses to stimuli below the injury cause vasoconstriction and hypertension, but
- an incomplete compensation of parasympathetic actions causes bradycardia and vasodilation above the injury.
Lumbosacral and Cervical Radiculopathy
The spinal nerve roots are immediately peripheral to the spinal cord with which they communicate (afferent and efferent--entering and exiting, respectively). Some lifting or lifting + twisting motions can challenge the integrity of the joint to maintain the disc(s) in the proper position. In these cases, a sudden herniation of a disc can present as an acute impingement of a nerve root, causing what are called "lumbosacral or cervical (most common sites) radiculopathies."
(Chronic radiculopathy can progress over time from bone spurs and spinal stenosis.)
Symptoms of Radiculopathy (along the path of nerve supplied by a particular nerve root):
- Pain.
- Numbness.
- Tingling.
Special Assessment Considerations
NEUROLOGICAL EXAM: A neurological exam is the standard assessment used to characterize a spinal cord injury, consisting of:
- sensation,
- strength, and
- reflexes.
You can expect a total injury to exhibit a "sensory/motor level" below which no sensation/voluntary function exists. Keep in mind that partial injuries may initially present as total injuries due to spinal shock.
SENSATION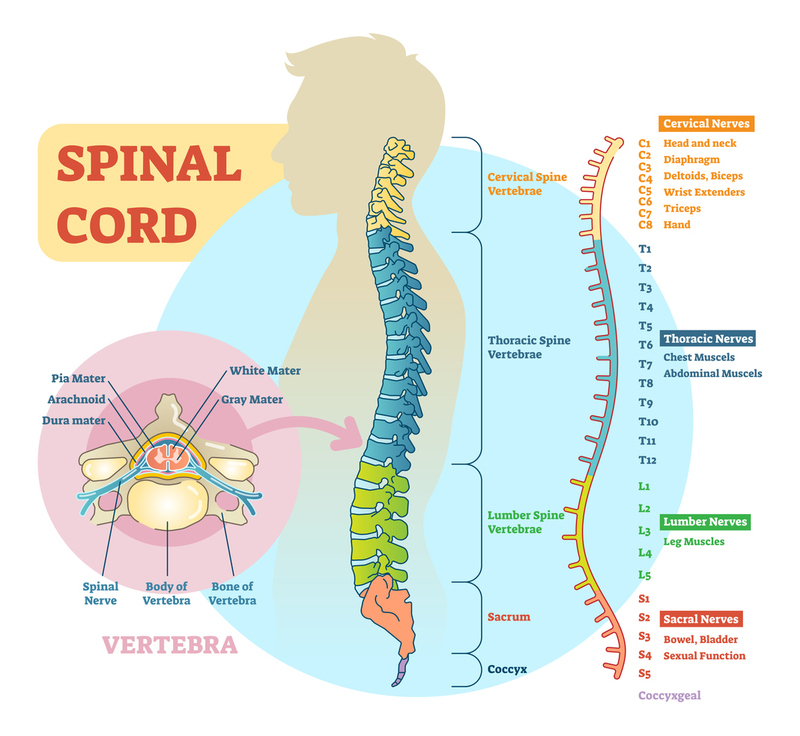
Sensation is assessed through dermatomes--regions in the skin known to send sensation to the brain through the nerves at specific vertebrae.
►The important dermatomes to memorize are
- C3, C4, and C5 for the diaphragm;
- C6, C7, and C8 at the hands;
- T4 at the nipples and
- T10 at the umbilicus.
STRENGTH
Strength is graded on a scale 0 - 5:
- 0 being total lack of strength,
- 3 being movement against gravity only, and
- 5 being full strength.
1, 2, and 4 are shades of gray.
REFLEXES
Reflexes should be assessed as they can elucidate the presence of spinal shock.
- Absent reflexes or "flaccid paralysis" is present in peripheral nerve damage and spinal shock.
- Acute transection can cause spinal shock, with a flaccid paralysis, urinary retention, and diminished tendon reflexes.
This is usually temporary, and increased tone, spasticity, and hyperreflexia will usually replace it a few days later. With the onset of hyperreflexia, "spastic paralysis" is present.
VITAL SIGNS are important due to the possibility of hypotension, hypothermia, and bradycardia secondary to sympathetic (autonomic) nervous system dysfunction as discussed above.
Special Management Considerations
Spinal immobilization is the key tenet of treatment for suspected spinal cord injuries. Cervical collars, full-length backboards, and log roll movements are the standard of care.
IV bolus of normal saline is the initial treatment for hypotension secondary to spinal cord injury, i.e., neurogenic shock.
- Maintaining a mean arterial pressure > 90mmHg systolic is required.
- Vasopressor support is indicated if fluid resuscitation cannot maintain blood pressure.
- Both chemical and physical options should be considered (pneumatic anti-shock garment).
Steroids: Prompt administration (within 8 hours) of corticosteroids has been shown to improve neurological recovery by reducing nerve edema and neuronal death.
In some cases these may be administered in the field, the standard dose being an IV bolus of methylprednisolone 30mg/kg.
It is important to remember that steroids cause worse outcomes in TBI patients, so if TBI cannot be ruled out, steroids should never be given. Any signs or symptoms that occur in the face or with pupillary changes or eye movements generally mean there is also a TBI.
Other Relevant Conditions
There are other medical conditions that can mimic spinal cord injury, generally, the giveaway that one of these conditions is at fault is the lack of recent trauma in an otherwise healthy patient. The two that are encountered most commonly in the EMS setting are Gullian-Barre syndrome (GBS) and Multiple Sclerosis (MS).
GBS results from a bacterial or viral infection and causes a rapid ascending flaccid paralysis that develops over the course of days, it is a medical emergency as it can compromise the diaphragm and prevent proper respiration. Unlike spinal cord damage sensation and vascular tone are generally unaffected.
MS is an autoimmune disease that attacks the myelin of the nerves in the cental nervous system. When this affects a segment of the spinal cord it is called "transverse myelitis" and can have any number of effects. The "flare" of MS will generally develop over days to weeks and results in a progressive weakness/paralysis of certain areas.
The treatment for both of these special conditions is management of the ABC's and transport to emergency care. EMS activation is generally rare for these conditions as patients seek medical care long before the conditions become life-threatening.