Test Complete
- Questions
- Score
- Minutes
| Overall Results | |
|---|---|
| Total Questions |
| Category Results | |
|---|---|
ABC vs CAB
Category: Cardiology
Topic: Cardiac Arrest
Level: EMR
Next Unit: Quick And Dirty Guide To Working A Cardiac Arrest
12 minute read
ABC vs CAB: Which is Correct?
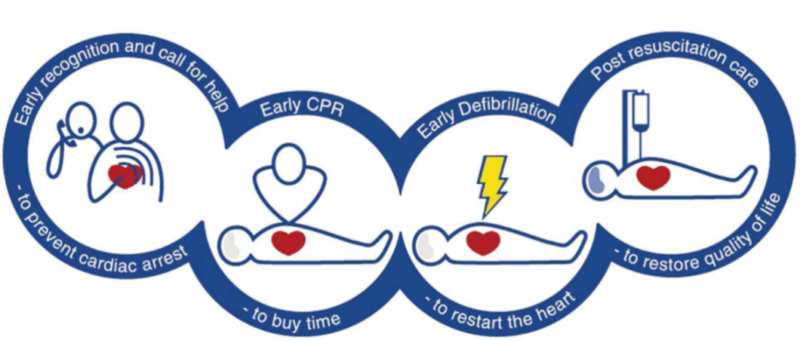
In 2010 the AHA made a radical change to how we approach CPR. Up until then, we all lived by the trusty "ABC" (Airway, Breathing, Circulation) method of resuscitation. Not surprisingly, though, the AHA's ongoing research began to show that compressions are the most important part of CPR and any delay or interruption resulted in worse outcomes. It was also discovered that during CPR, the patient's blood stays oxygenated for 4-6 minutes after their last breath. In response to this research, and in an attempt to simplify CPR for untrained laypeople, the AHA decided to switch our initial approach from ABC to CAB. While this change is medically sound, it has caused a lot of confusion for healthcare professionals who regularly use ABC for other scenarios. So, ABC vs CAB, which is correct? This post will explain the history of both approaches and when it is appropriate to use one over another.
ABC - Old School
In 1973 the ABC model, originally popularized by Peter Safar, was adopted by the AHA as a mnemonic for first-aiders to remember the steps of CPR. Over time, the ABC assessment was informally adopted by the emergency medicine crowd as the unconditional first step during an assessment. ABC has fit the bill for the unique environment of emergency medicine because of its simplicity and its ability to immediately identify life threats. Since its inception, we've happily used this mnemonic in every situation, from childbirth to chest pain.
CAB - New School
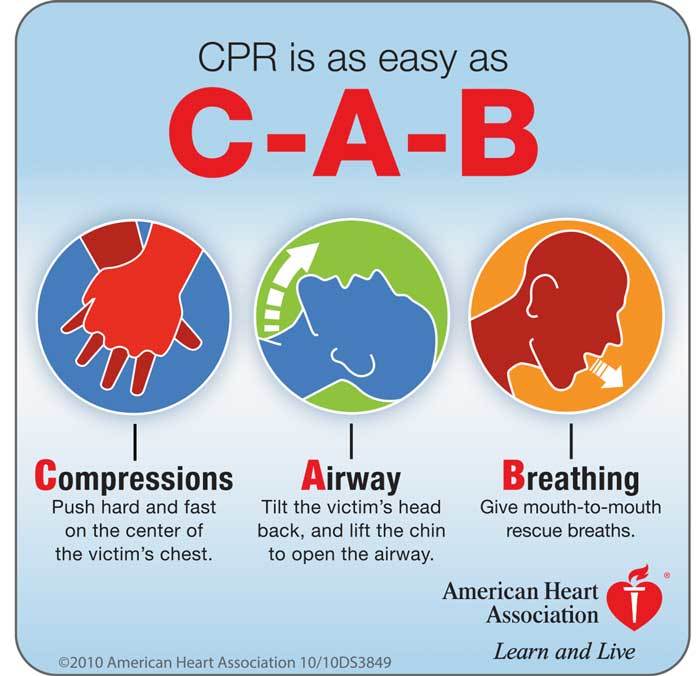
With indisputable evidence that compressions are the most important part of CPR, it is no wonder that AHA has been de-emphasizing airway and breathing. In fact, in ACLS, the AHA has gone as far as to suggest that endotracheal intubation may not be as important as we once thought. While it remains the ultimate airway, the AHA suggests BVM or supraglottic airway ventilation because they reduce the interruption of compressions.
The MARCH algorithm, often synonymous with Tactical Combat Casualty Care (TCCC), prioritizes Massive hemorrhage, Airway, Respiration, Circulation, and Hypothermia/Head injury, reflecting a shift from the traditional ABC (Airway, Breathing, Circulation) approach. This change has been influenced by military medicine and trauma care research, emphasizing the importance of controlling severe bleeding before addressing airway issues in certain trauma scenarios, especially in polytrauma patients where life-threatening hemorrhage is present.
XABC in Trauma: Why, What, How
Why Switch From ABC to XABC? In severe trauma, uncontrolled bleeding can kill a patient before airway or breathing issues become the limiting factor. Without circulation, the airway does not matter because there is no blood to carry oxygen.
What XABC Means
- X – Exsanguination control: Stop catastrophic bleeding immediately
- A – Airway
- B – Breathing
- C – Circulation (still essential, but after airway and breathing unless massive bleeding is present)
How to Apply It in the Field
Identify life-threatening bleeding within seconds of patient contact
- Control the bleeding immediately using tourniquets, hemostatic dressings, or direct pressure
- Secure the airway once bleeding is under control
- Support breathing and oxygenation
- Restore circulation with rapid and targeted resuscitation
In trauma scenarios with severe bleeding, the XABC sequence is used instead, emphasizing exsanguination control (X) before airway management. The "C" in CAB can also be applied to a trauma scenario, as it refers to circulation. Think “bleeding before breathing.” We replace ABC with an evidence-driven plan: control hemorrhage first, then resuscitate without delay. Early action on circulation is the fastest way to keep trauma patients alive.
In accordance with this paradigm shift, the AHA has changed ABC to CAB in the event of cardiac arrest. Unfortunately, though, some healthcare providers have incorrectly interpreted this change in cardiac arrest to be a change that applies to every other medical call. Some are under the impression that the AHA is the governing body over prehospital and emergency care, which is simply not the case.
Here is a short list of examples of when ABC vs CAB vs XABC should be used!
ABC
- Overdose
- Altered mental status
- Diabetic emergencies
- Respiratory failure
- Airway obstruction
- Respiratory Distress
CAB
- Trauma - Control massive bleeding first!
- Unresponsive patient
- Cardiac Arrest
XABC
- Severe bleeding from penetrating trauma
- Traumatic amputation with uncontrolled arterial bleed
- Blast injury with limb trauma
- Multi-system trauma with significant blood loss
- Pelvic fracture with heavy bleeding
- Junctional hemorrhage (groin, neck, axilla)
Conclusion
CAB is now being used during cardiac arrest to remind practitioners and laypeople of the importance of compressions. In general, it is not useful to confine yourself to one ideology "because they say so." It is much more productive to understand each approach and use critical thinking to choose the best route for your patient.