Test Complete
- Questions
- Score
- Minutes
| Overall Results | |
|---|---|
| Total Questions |
| Category Results | |
|---|---|
A&P of the Brain and Spine
Category: Trauma
Topic: Nervous System Trauma
Level: EMT
Next Unit: Assessment Considerations for Brain Trauma Patients
34 minute read
Spine
SPINE: The spine is made up of individual vertebrae. They articulate with each other, forming a giant joint that protects the spinal cord while also allowing rotation, flexion, and extension. Spinal segments are named with a letter and number, e.g., C1, C6, T10, L3. Understanding the basic anatomy of the spine is essential for the management of trauma.
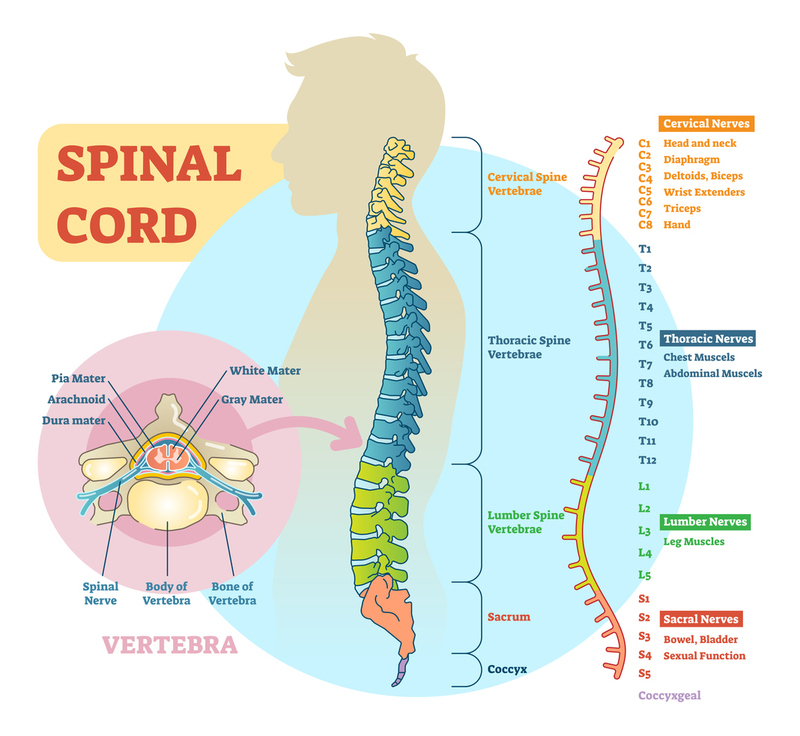
VERTEBRAE:
CERVICAL: C1 C2 C3 C4 C5 C6 C7
THORACIC: T1 T2 T3 T4 T5 T6 T7 T8 T9 T10 T11 T12
LUMBAR: L1 L2 L3 L4 L5
SACRAL: Fused S1/S2/S3/S4/S5
COCCYX: Fused 4 vertebrae
DEFINITIONS:
SPINOUS PROCESS: The protrusion from the rear (dorsal aspect) of each vertebra which acts as an anchor point for the muscles of the back.
CERVICAL SPINE: named C1-C7 and are the uppermost 7 vertebrae that make up the neck and base of the skull.
C1, called the ATLAS, and C2, called the AXIS, together support the head.
C7 is an important landmark located at the lower part of the neck above the thoracic spine.
Note that there is a "C-8" nerve, exiting under the last cervical vertebra (C-7). This can cause confusion in that there are 7 cervical vertebral segments but 8 cervical nerves.
THORACIC SPINE: named T1-T12, these middle 12 vertebrae have rib attachments that form the rib cage, providing protection to vital organs and limiting excessive spinal movement.
T4 is the level of the nipples, and
T10 is the level of the belly button (navel, umbilicus).
LUMBAR SPINE: named L1-L5, the lower 5 true vertebrae (below the ribs). These vertebrae bear the entire weight of the upper body and provide stability while allowing a range of motion, such as bending and twisting. The lumbar spine also protects the lower end of the spinal cord and nerve roots, with the spinal cord ending near L1-L2 and continuing as the cauda equina below this level.
SACRAL SPINE: named S1-S5, the sacral spinal processes are fused bony projections along the midline of the sacrum, forming the median sacral crest. They provide important sites for ligament and muscle attachment that stabilize the lower spine and pelvis. The sacrum connects the lumbar spine to the pelvis, supporting body weight and facilitating movement.
COCCYX (Tailbone): The coccyx, commonly known as the tailbone, is generally composed of four fused coccygeal vertebrae. This bone plays a role in weight-bearing when sitting and serves as an attachment point for pelvic ligaments and muscles. The coccyx articulates superiorly with the sacrum and typically fuses with it later in life.
CEREBROSPINAL FLUID (CSF): circulates up to the brain in the intrathecal space (space that holds the spinal cord), through the brain sinuses, then back down around the spine again. Running in the center of and around the spinal cord, this fluid is the same as that which cushions the brain. It is both produced and resorbed in a balance and cushions the brain from impacts against the skull.
SPINAL CORD: a collection of nerves that communicates information to and from the brain and to and from the remainder of the body. It is considered a component of the central nervous system (CNS).
SPINAL FORAMINA (singular, foramen): the holes along each spinal vertebra that allow the exit for the nerves originating from the spine.
Its nerve delineations are according to the vertebral segments, but its length is skewed shorter, meaning the actual cord ends at about L2, with the remainder of the nerves (associated with L2 downward having to run inferiorly to reach their respective foramina, bunched together as the cauda equina, or "horse's tail."
SCOLIOSIS: lateral (sideways) curvature of the spine.
KYPHOSIS: abnormal convexity of the spine ("hunch back").
LORDOSIS: abnormal inward curvature of the lower spine ("swayback").
Spinal Cord Injury
LEVEL OF SPINAL CORD INJURY: Damage to the spinal cord and its associated vasculature is a feared complication of any traumatic injury. Spinal cord injury that interrupts the signal from/to the brain to that part of the body associated with that spinal segment will manifest according to the level of spinal cord injury:
C1 - C4: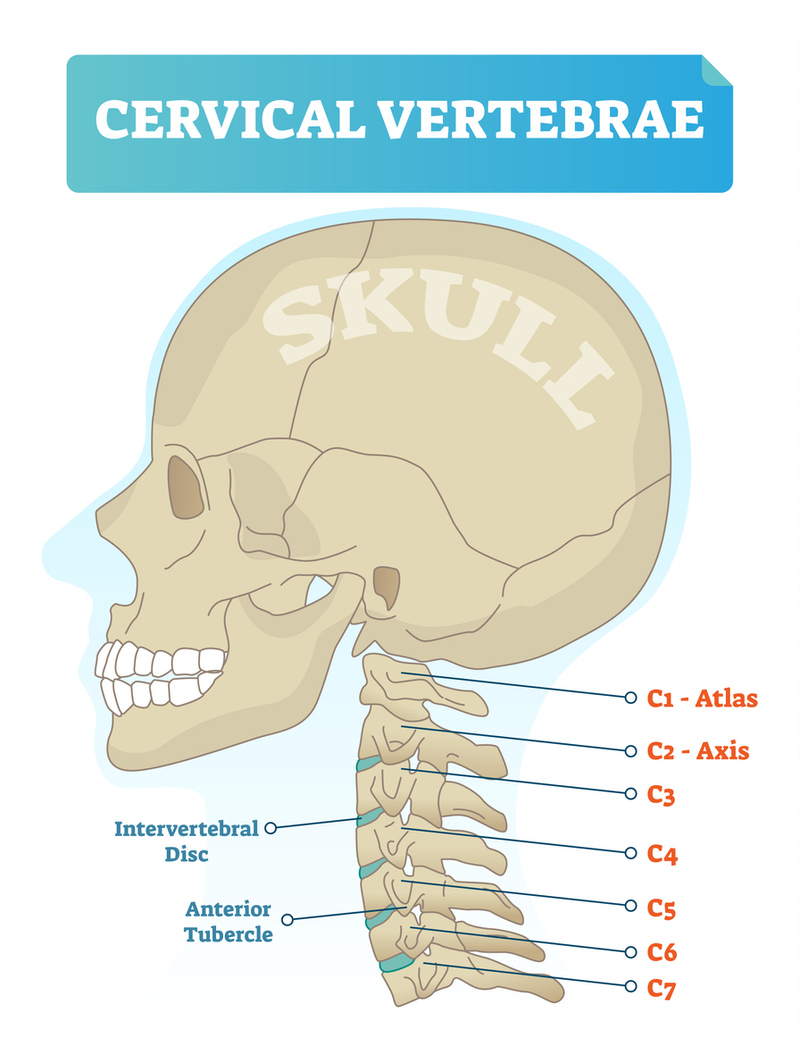
- Considered a high spinal fracture.
- Most severe of the spinal cord injury levels.
- Results in paralysis in arms, hands, trunk and legs.
Quadriplegia--all four limbs affected.
A patient may not be able to breathe on his or her own, cough, or control bowel or bladder movements, and speech may be impaired.
C5-C8:
- The nerves that control the arms and hands
- Breathing is weakened
- Little or no voluntary control of bowel or bladder
T1-T5:
- Nerves for upper chest, mid-back and abdominal muscles. (Arm and hand function is usually spared).
- Affects the trunk and legs (also known as paraplegia).
T6-T12:
- Nerves for abdominal and back muscles.
- Usually results in paraplegia, with normal upper-body movement.
- Should be able to cough productively (if abdominal muscles are intact).
- Little or no voluntary control of bowel or bladder.
L1-L5:
- Loss of function in the hips and legs.
- Little or no voluntary control of bowel or bladder.
S1-S5:
- Loss of function in the hips and legs.
- Little or no voluntary control of bowel or bladder.
Coccyx (tailbone)
- No spinal cord involvement
In the field, the noteworthy assessment is whether speech and breathing are impaired. If so, suspect a high cervical fracture.
Brain
DEFINITIONS:
SKULL: The skull is made up of many individual bones, coming together after birth in areas called suture lines, which fuse to act as one large bone, protecting the brain, eyes, and oral/nasal passages.
MENINGES: The 3 meningeal layers cover the brain and spinal cord, keeping them separate from the rest of the body. They also act to contain the CSF, which acts as a shock absorber for the brain and spinal cord.
![]()
The meninges are part of the blood-brain barrier (BBB), responsible for filtering out bacteria, viruses, and even some medications from passing from the body into the intrathecal space (spine and brain).
- Dura mater: the outermost layer, a tough tissue layer that lies directly beneath the bone of the skull and spine. This layer contains many veins that drain the brain and spine.
- Arachnoid mater: the thin and friable middle layer, connects directly to the bottom of the dura mater. This layer does not contact the pia mater; there is an empty space between the arachnoid and pia mater layers in which the CSF circulates.
- Pia mater: the innermost layer, an extremely thin membrane that lies directly on the surface of the brain/spine.
GRAY MATTER: The cell bodies of the neurons in the brain and spine, responsible for generating/propagating electrical signals. Gray matter is found throughout the brain and in the center of the spinal cord.
WHITE MATTER: The long "wires" (axons) that connect the grey matter to other grey matter or to the peripheral nerves. It is “white” due to the large amounts of fat (myelin) that acts to insulate the axons. White matter is found between major areas of the brain and the periphery of the spinal cord.
In the spinal cord, the gray matter containing the neuronal cell bodies occupies a butterfly-shaped central region, and the white matter tracts surround it.
In the brain, white matter is made of axons connecting different parts of gray matter to each other.
BRAINSTEM: The brainstem is responsible for maintaining homeostasis, regulating almost every function that keeps our bodies alive, e.g., heart rate, breathing, temperature, plus all gastrointestinal (GI) and genitourinary (GU) functions.
CEREBRUM: The cerebrum is responsible for consciousness and the processing of 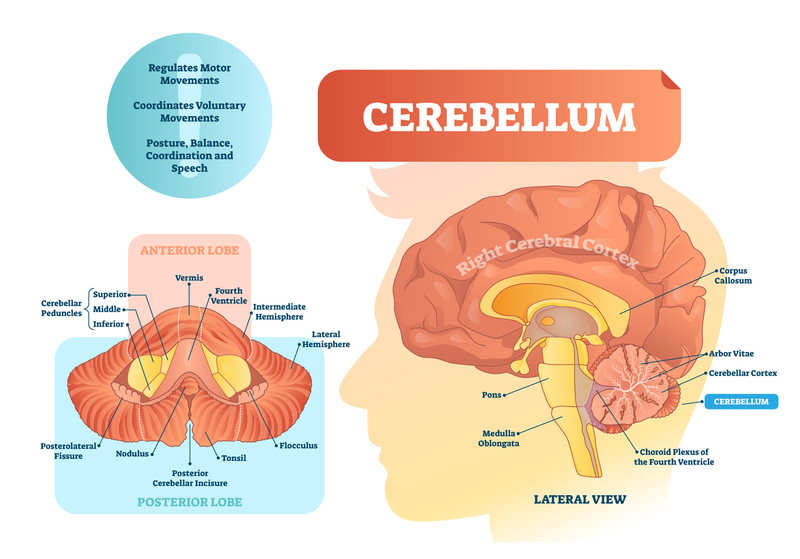 information, known as “higher brain functions.” It is divided into mirrored right and left sides, with four named lobes on each side:
information, known as “higher brain functions.” It is divided into mirrored right and left sides, with four named lobes on each side:
- frontal,
- temporal,
- parietal, and
- occipital.
CEREBELLUM: Latin for “small brain,” located below the occipital lobe at the base of the brain behind the brainstem. Responsible for fine motor movements and coordination of multiple muscles to create a single smooth action.
Types of Skull Fractures
BASAL (Basilar): a fracture of the bones that make up the base of the skull, most commonly the temporal bone; commonly includes rupture of the meninges and leakage of CSF.
- Will present with raccoon eyes,
- bruising behind the ears, and
- leakage of CSF or blood from ears and nose.
It is a must-not-miss diagnosis, which can rapidly lead to death. There is really nothing else (other than a penetrating injury to the ear, e.g., pencil, etc.) that can cause blood to be seen coming from the ear(s).
The Halo Test: Bloody discharge from the nose or ears can have CSF in it. The Halo Test involves just observing the blood drop on linen. Since blood is more viscous than CSF, the CSF expands beyond the border of the blood drop, resembling a halo. Absence of a halo does not rule out a basal skull fracture: any blood from the ears is considered a basal skull fracture till proven otherwise (after arrival at a facility).
COMPRESSED: a depression or sunken-in spot on the skull, usually secondary to blunt force trauma and often associated with
- epidural or subdural bleeding which can result in increased intracranial pressure (ICP),
- brain compression, and
- death even in patients who initially recover.
OPEN: removal of a portion of skull leading to exposure of the brain or meninges, most commonly secondary to penetrating trauma.
- High risk for infection, it may be associated with a deeper injury that is not initially obvious.
- Any skull injury that is draining clear or yellow fluid (CSF) in conjunction with blood should be considered an open fracture.
LINEAR: most common skull fracture--a simple line through the entire thickness of the skull.
- It usually goes unnoticed until the patient is imaged, often unimportant compared to the traumatic brain injury (TBI) that may have occurred from the same injury.
- As in compressed fractures, linear fractures may result in bleeding beneath the skull.
Brain Injuries
Brain injuries have a varied presentation; however, no matter the injury, certain signs and symptoms warrant further medical evaluation:
- “evolving” deficits, i.e., worsening confusion/weakness; and
- “focal” signs, e.g., one abnormal pupil, weakness in ½ of the body, or loss of consciousness.
DEFINITIONS:
CONCUSSION: The mildest form of traumatic brain injury, commonly due to blunt force and resultant compression of the brain against the inside of the skull. Defined by short-lived neurological impairments:
- confusion,
- amnesia,
- agitation, or
- somnolence.
An acute headache, nausea, vomiting, and ataxia are common. Loss of consciousness is considered a red flag and requires imaging. These patients must be observed for 24 hours following the injury to watch for evolving deficits.
NOTE: Post-concussion syndrome--Adults with a diagnosis of concussion had an increased long-term risk of suicide, particularly after concussions on weekends (no kidding).
CONTUSION: “bruising of the brain,” usually secondary to blunt force injury. Contusions can present with symptoms as mild as a headache all the way to coma and death, and can progress from mild to severe symptoms over minutes or hours.
Assessment should focus on suspicion for increased intracranial pressure (ICP), most commonly presenting with:
Nausea, vomiting,
confusion,
headache, and
changes in vision/pupils.
TRANSTENTORIAL HERNIATION: the most feared complication of ICP, presenting with
pupillary changes,
significant changes in consciousness,
strange posturing (obtundation), and
death.
CEREBRAL LACERATION: Rare, usually associated with penetrating trauma.
- Symptoms can vary widely based on the location of injury.
- Any foreign object(s) protruding from the skull should be stabilized and left in place.
- Watch for signs of increased ICP listed above.
SPACE-OCCUPYING LESIONS:
- Most commonly tumors and blood clots, commonly presenting with symptoms of increased ICP as listed above, or at worst, transtentorial herniation.
All patients with head trauma require repeat evaluations to rule out formation of a space-occupying lesion.
INTRACRANIAL BLEED
- EPIDURAL BLEED: This is the most common space-occupying lesion.
- Bleeding from the meningeal arteries forms a “lens-shaped” (concave) mass between the skull and the dura mater.
- The typical picture is a young individual with a concussion who passed out briefly and rapidly, recovered at the scene (lucid interval), then 1-2 hours later he/she begins getting sleepy which progresses to unresponsiveness and the signs of a space-occupying lesion appear as listed above.
- SUBDURAL BLEED: Bleeding from the veins that cross the meninges.
- Essentially less severe than an epidural bleed.
- Not arterial, so it progresses more slowly.
- The typical picture is an elder who falls and hits his/her head, has no loss of consciousness, but begins acting confused/agitated/somnolent after 2-20 weeks. A CT scan will reveal a mass that “hugs” the contours of the brain.
- This is commonly mistaken for dementia by family/friends/care providers.
- Red flag for child abuse: in children, other than an MVA, abuse is usually the cause.
EPIDURAL vs SUBDURAL BLEED
- Epidural bleeding is typically arterial.
- Subdural is typically venous.
- Epidural bleeding is more acutely serious.
- Subdural bleeding progresses more slowly.
- Epidural bleeding cannot cross "suture lines," because it is blocked by the falx cerebri--a downward reflexion of the dura mater that dives between the right and left cerebral hemispheres, but is anchored to the skull above (under the suture line). Therefore, all bleeding is compartmentalized and limited by the dura's attachment to the skull. It is this arrangement of anatomy that produces a "midline shift" of the brain on imaging studies.
- Subdural hematomas can cross suture lines, bleeding under and following a route similar to CSF circulation.
- Epidural bleeds are usually due to a strike to the head (sports, etc.)
- Subdural bleeds, especially in children, are usually due to child abuse (skull fractures, shaking).